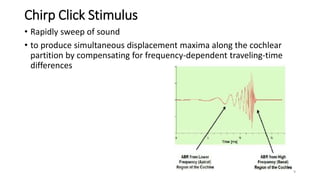
This document discusses various parameters for auditory brainstem response (ABR) testing, including stimulus type, intensity, and presentation rate. It describes advantages and disadvantages of different transducer types (insert earphones, supra-aural earphones, bone vibrators) and stimulus types (clicks, tone bursts, chirps, speech). Factors that influence ABR waveforms like latency and amplitude are discussed in relation to stimulus intensity, frequency, duration, and envelope. Guidelines are provided for optimal application of different stimulus parameters in clinical ABR testing.