

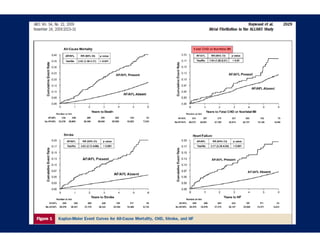
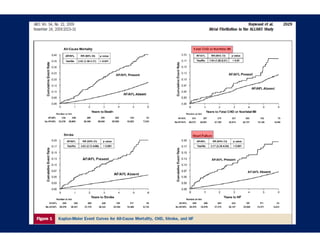
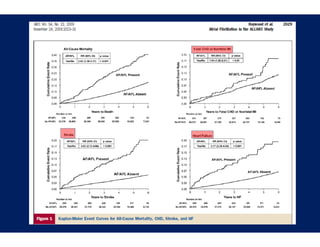
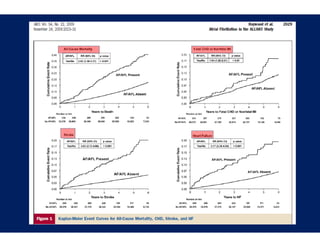
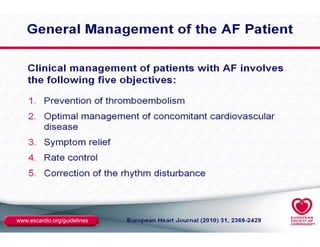

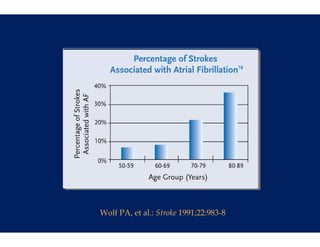
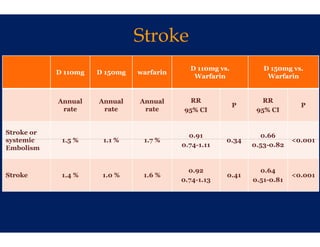
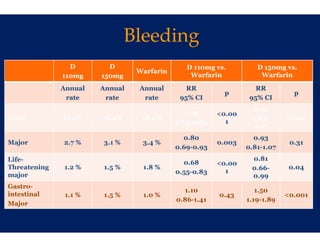
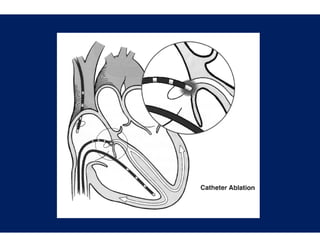

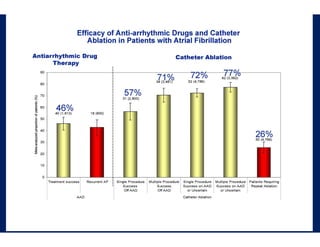
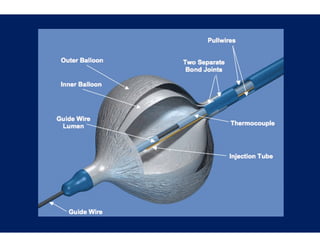
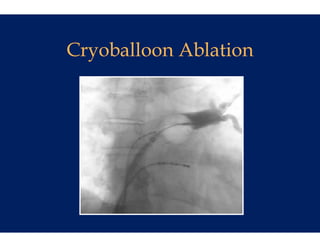

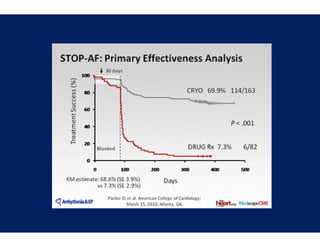
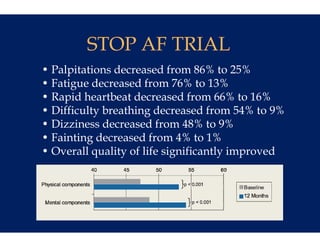
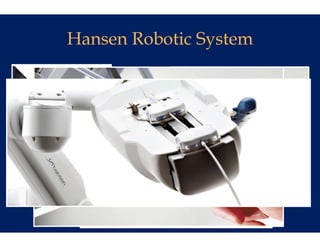
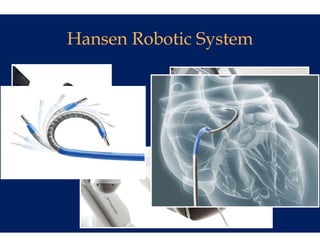
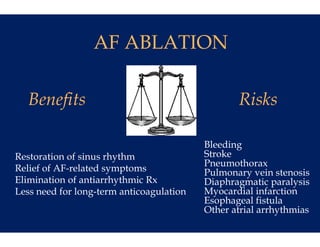

The document discusses recent advances in the management of atrial fibrillation (AF), including the use of anticoagulants like warfarin and dabigatran for stroke prevention, as well as catheter ablation therapies for maintaining sinus rhythm in symptomatic patients. It highlights studies demonstrating the effectiveness of these treatments and underscores the importance of experienced centers in performing catheter ablation to achieve optimal outcomes. The document emphasizes the significant public health implications of AF and the need for ongoing improvements in treatment strategies.











































































































