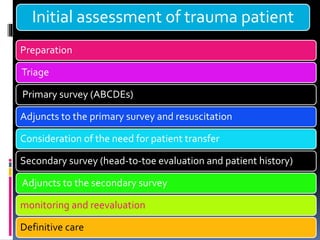
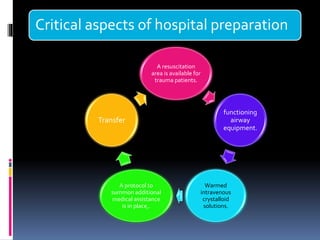
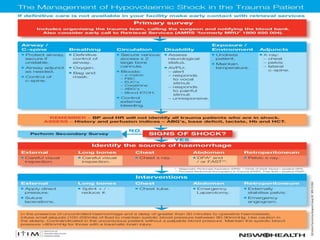
Initial assessment of a trauma patient involves a primary survey using the ABCDE approach to identify life-threatening injuries. For the described trauma scenario, the initial steps would be:
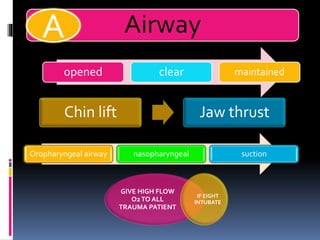
1) Assess the airway and give high-flow oxygen. The patient's ability to speak suggests his airway is not compromised.
2) Evaluate breathing and circulation. His breathing is compromised as shown by the low respiratory rate and high pulse.
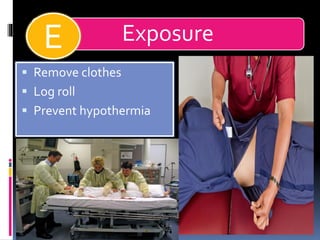
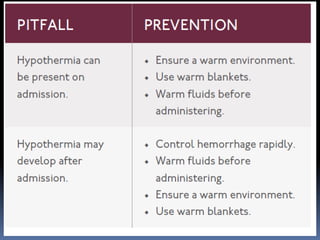
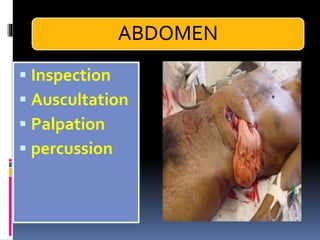
3) Expose the patient fully to identify injuries and monitor for hypothermia. The abrasion on his chest indicates potential internal injuries.
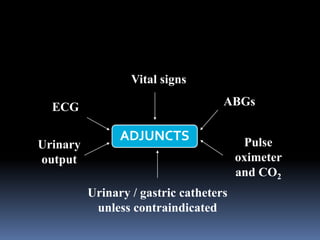
4) Begin resuscitation with IV fluids and monitor vitals closely given his unstable condition from potential internal bleeding and shock.
5)

































































![Approach_to_the_trauma_patient[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/approachtothetraumapatient1-220906191256-c4d92395-thumbnail.jpg?width=640&height=640&fit=bounds)
































