





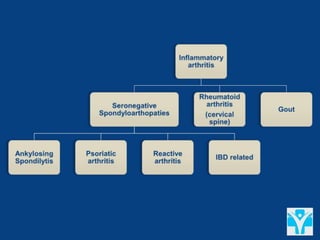

![IBD-related arthritis
Type 1 (arthritis parallels IBD activity) - 4% to 6% of IBD patients, acute in
onset, asymmetric; + extraarticular manifestations (erythema nodosum,
uveitis).
Most arthritic episodes are self-limited with 80% resolving within 3
months. This type of arthritis does not result in radiographic changes or
deformities.
Type 2 (arthritis is independent of IBD activity) - 3% to 4% patients;
symmetric (80%), polyarticular (metacarpophalangeal [MCP] joints >
knees and ankles > other joints), runs a course independent of the activity
of the inflammatory bowel disease](https://image.slidesharecdn.com/assessingbackpaininrheumatology-201106012924/85/Assessing-back-pain-in-rheumatology-27-320.jpg)

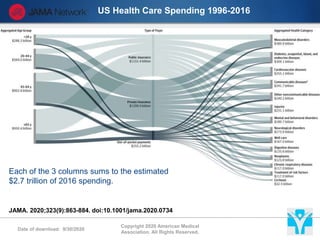
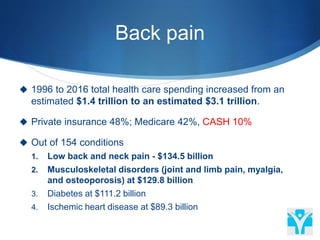
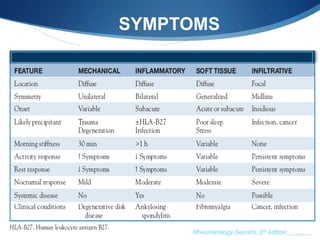
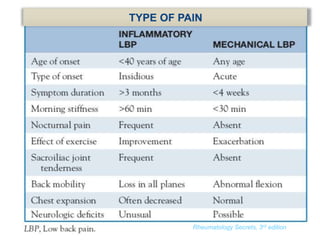
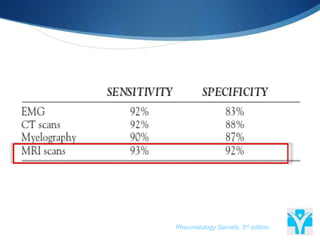
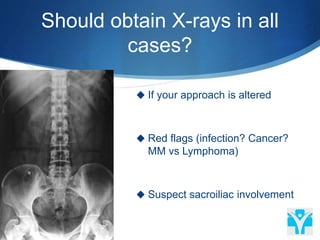
The document discusses back pain assessment from a rheumatology perspective, detailing healthcare spending related to back pain and common diagnostic approaches. It emphasizes that most low back pain is mechanical, outlines when imaging should be utilized, and highlights red flags and symptoms to consider. Management tips suggest prioritizing exercise and physical therapy, avoiding certain tests in the early stages, and providing guidelines for inflammatory arthritis treatment.























































































