Downloaded 39 times














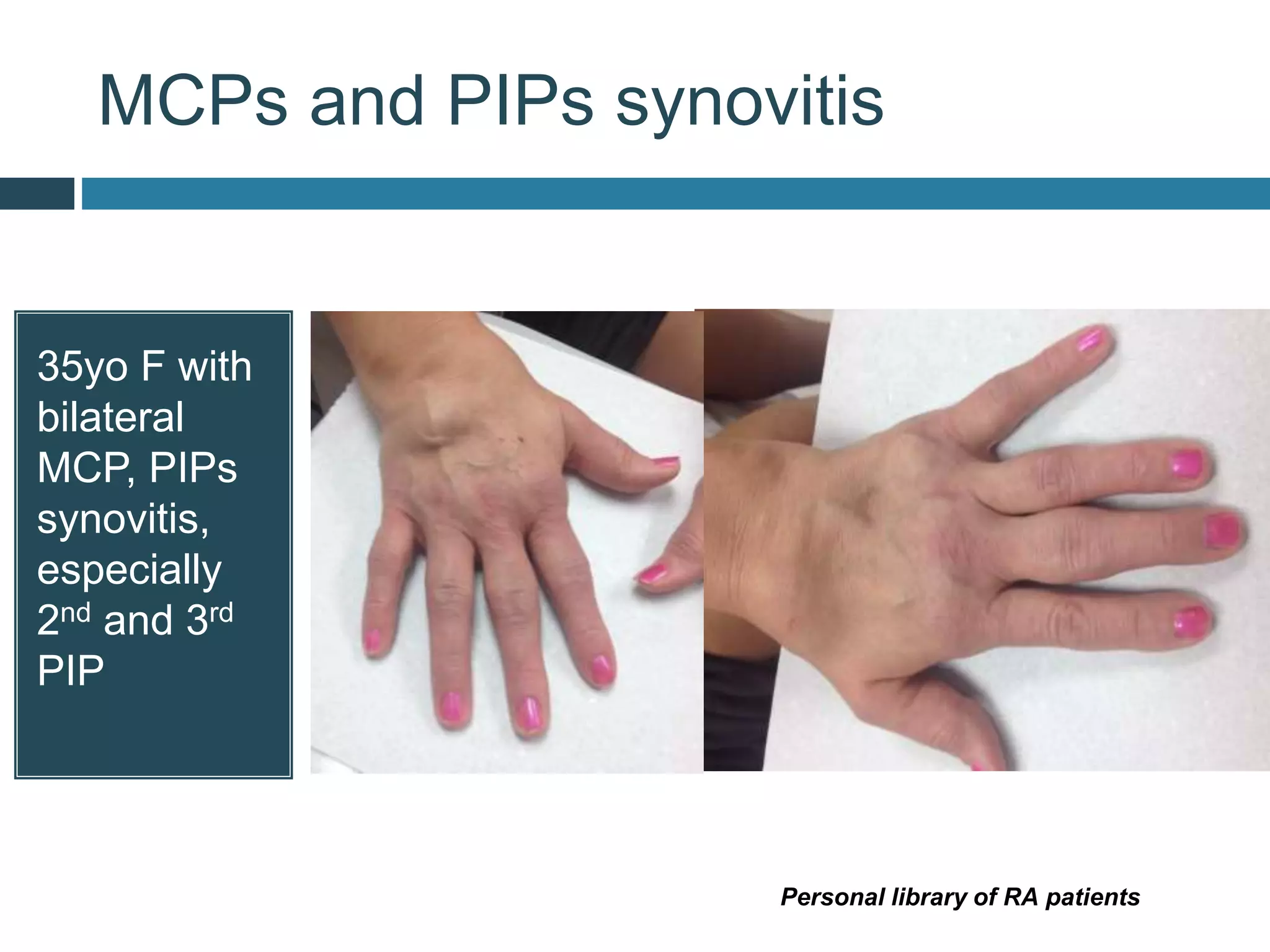



































































Rheumatoid arthritis is a common autoimmune disease that causes inflammation in the joints. It can lead to joint damage, deformity, disability, and reduced life expectancy if left untreated. It is characterized by symmetric inflammation of small and medium-sized joints. Extra-articular manifestations can include lung, heart, eye, and skin involvement. Diagnosis is based on symptoms, laboratory tests for rheumatoid factor and anti-CCP antibodies, and imaging of affected joints. Early, aggressive treatment is important to prevent long-term damage.























































































