Download to read offline
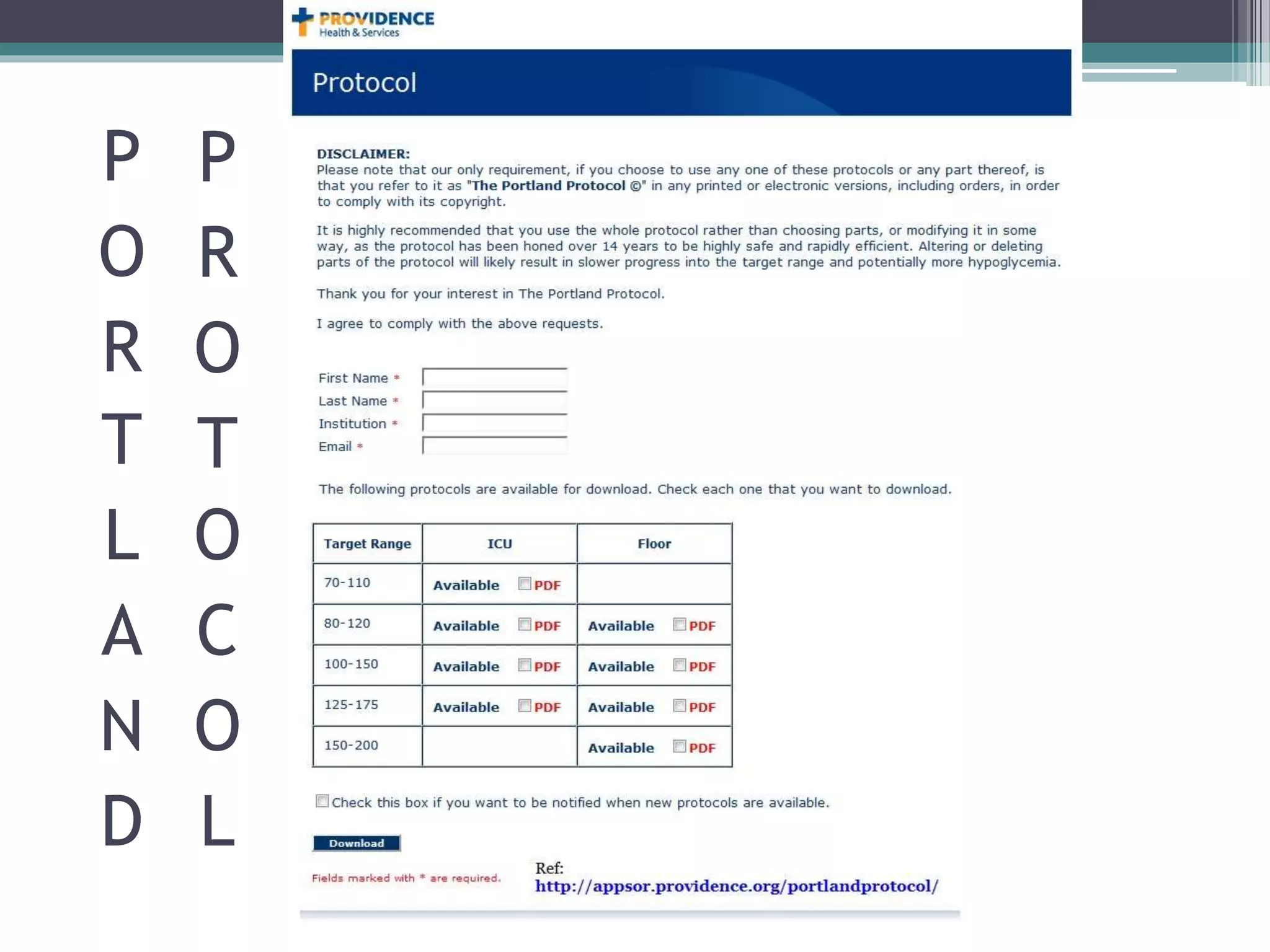
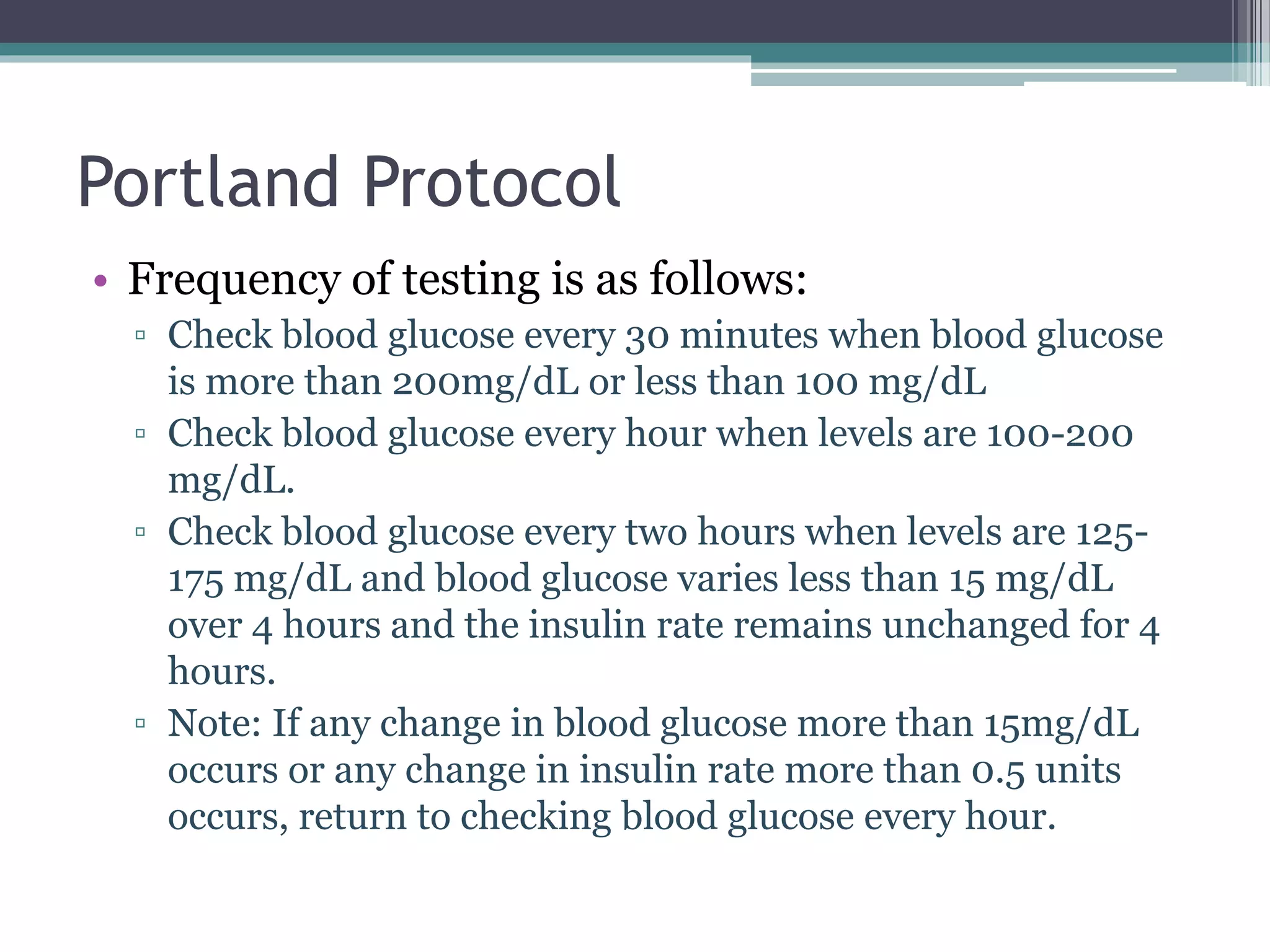
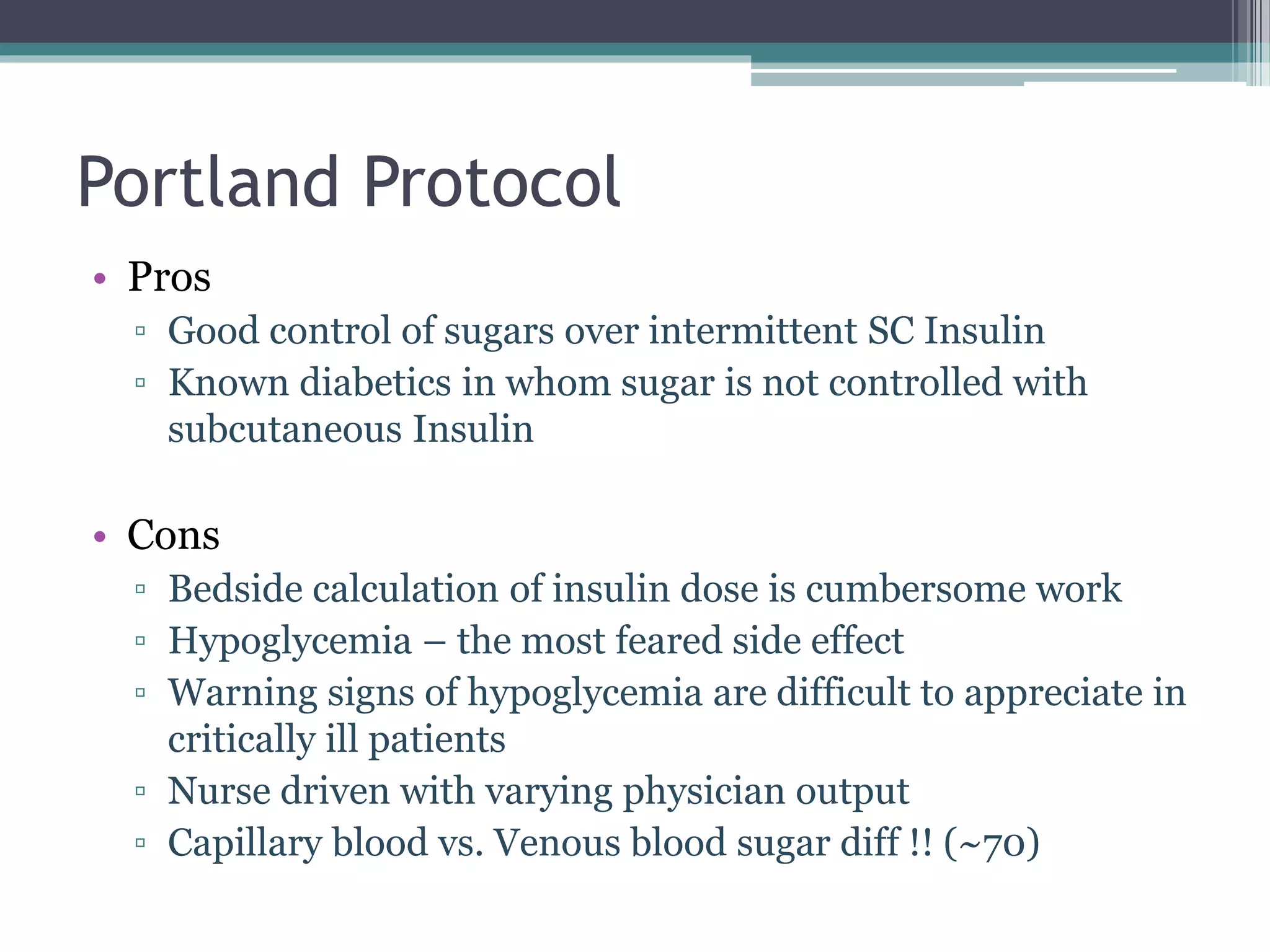

The document reviews the Portland Protocol for insulin therapy in critically ill patients, detailing the need for managing hyperglycemia to reduce morbidity and mortality. It outlines the protocol's development, clinical applicability, and specific blood glucose monitoring and insulin administration guidelines. The protocol aims for a target blood sugar range of 100-150 mg/dl and highlights both benefits and challenges in its implementation.