Downloaded 64 times

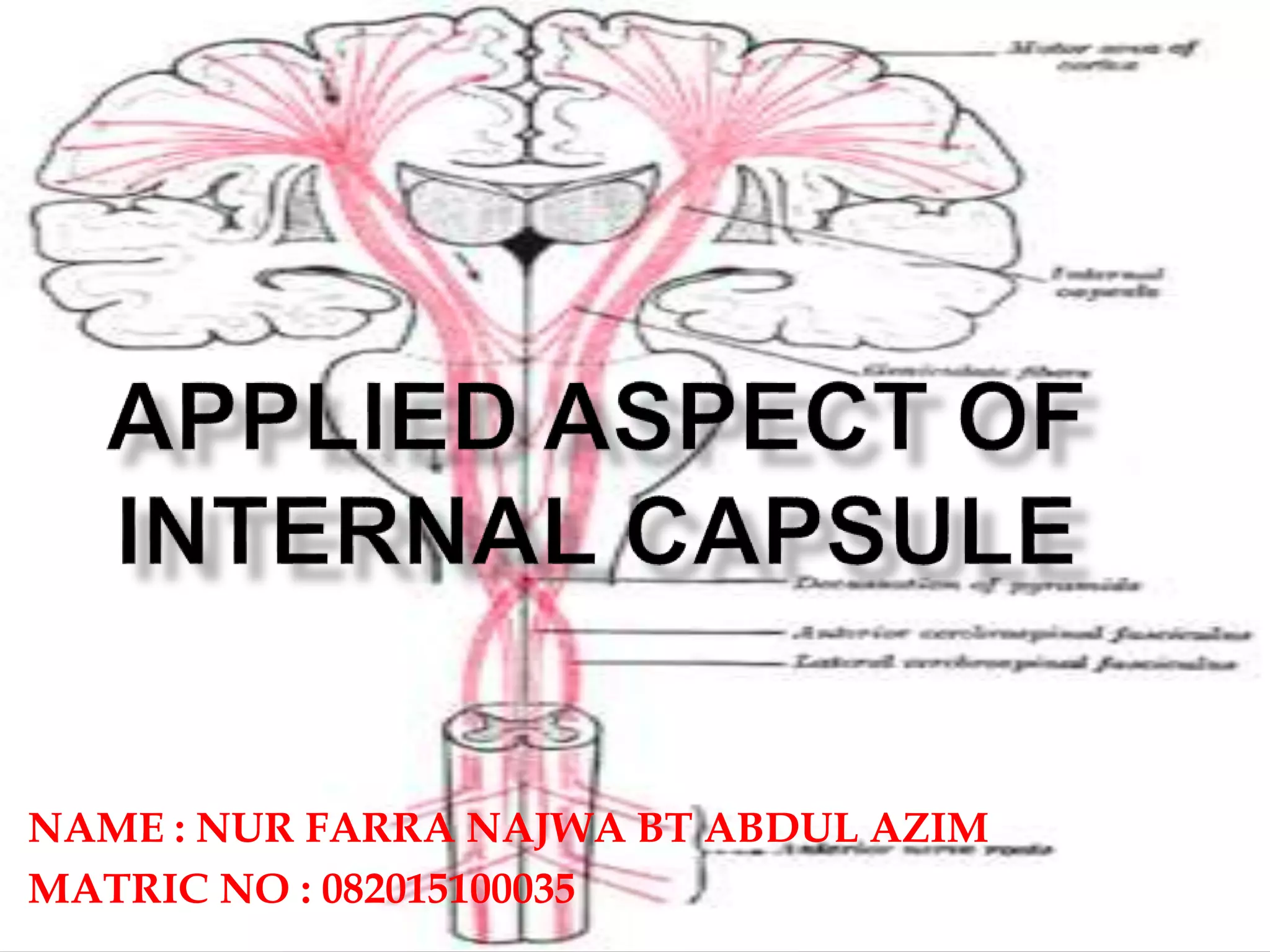
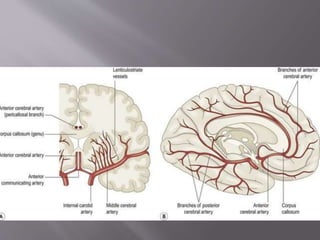

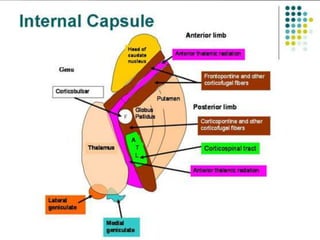
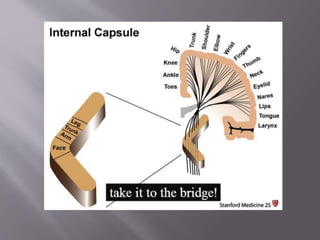
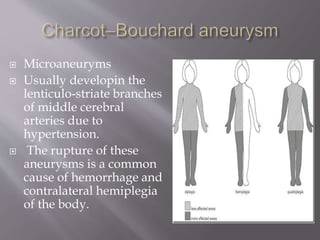
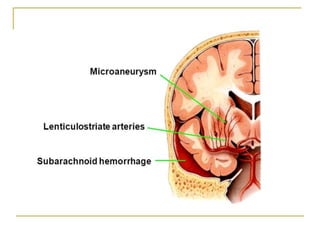
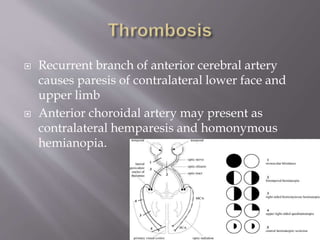
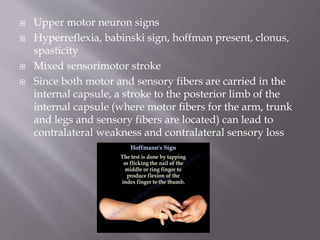


This document discusses the internal capsule, which carries motor and sensory fibers between the brain and spinal cord. It notes that lesions in different parts of the internal capsule can cause weakness or sensory loss on the contralateral side of the body. Small vessel disease from hypertension is a common cause of lesions in the internal capsule. Symptoms may include hemiparesis, hemiplegia, sensory loss, and upper motor neuron signs like spasticity, depending on the location of the lesion within the internal capsule.




















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


