Download to read offline



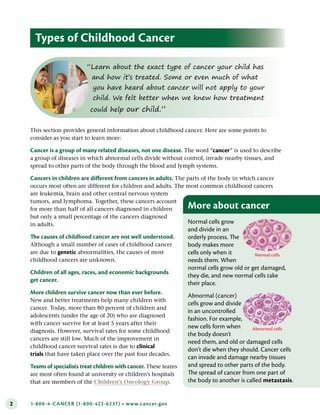















































































This document provides information for parents on diagnosing childhood cancer, including common symptoms, diagnostic tests and procedures used to identify the type and stage of cancer, the importance of having biopsies done at specialized hospitals, and questions to ask about tests and results to understand the diagnosis and plan treatment. It explains that childhood cancers are different than adult cancers and lists the most common types such as leukemia, brain tumors, lymphoma, and others.























































































