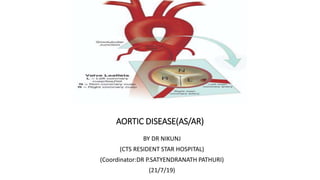
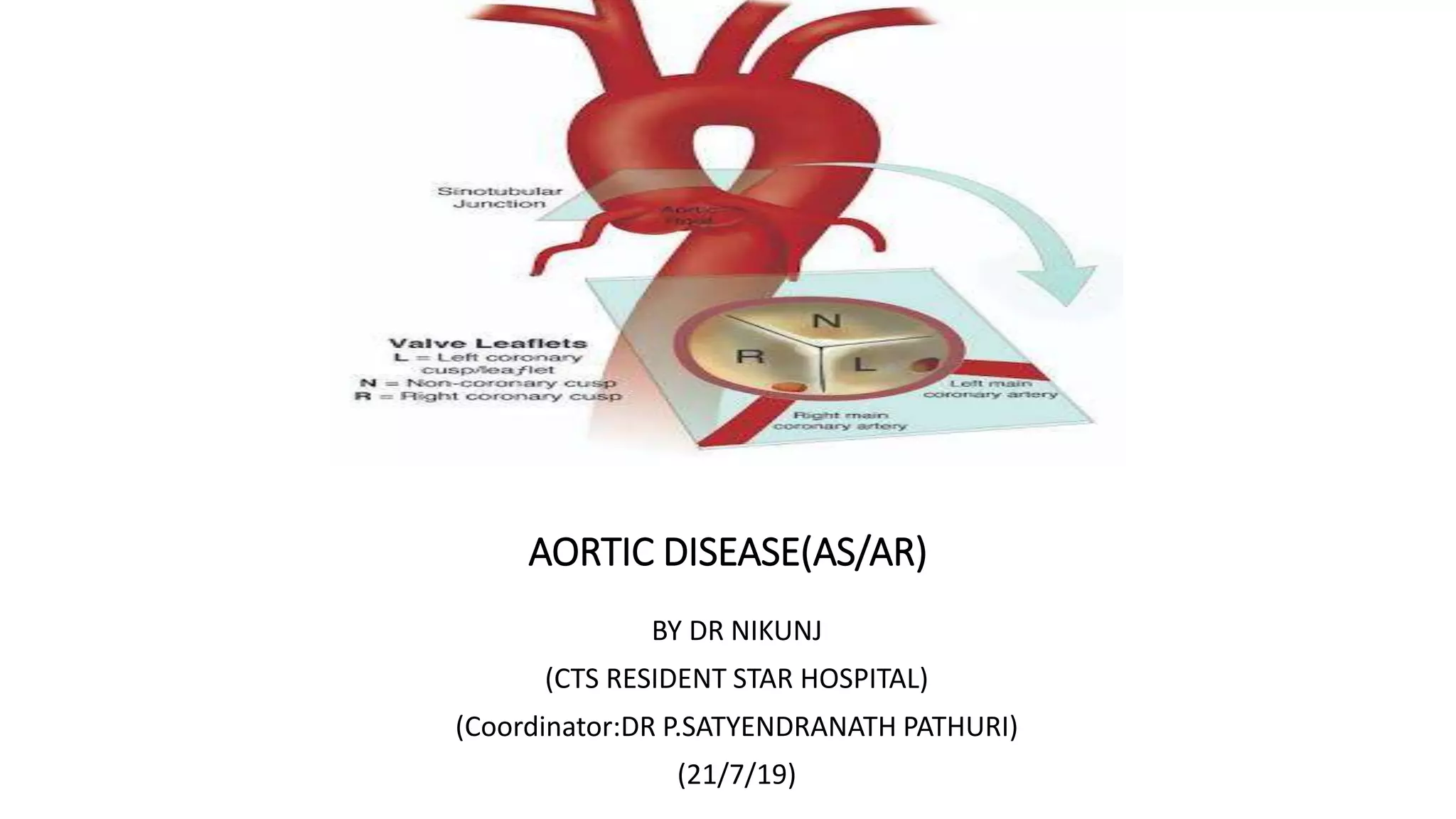
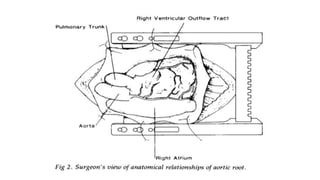
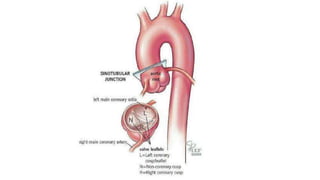
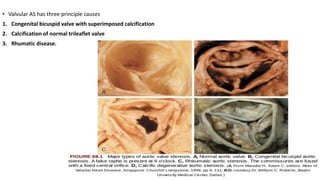
The document provides information on aortic valve disease including anatomy, etiology, and pathophysiology. It describes the key components of the aortic root including the aortic annulus, cusps, sinuses, and sinotubular junction. The three main causes of aortic stenosis are discussed as congenital bicuspid valve with calcification, calcification of a normal trileaflet valve, and rheumatic disease. The pathophysiology of aortic stenosis involves left ventricular pressure overload leading to hypertrophy and eventually decreased ejection fraction if severe stenosis is not corrected.