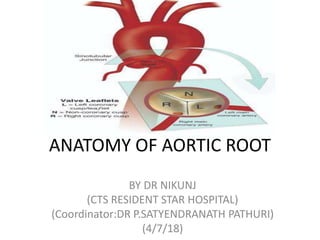
The aortic root connects the left ventricle to the ascending aorta and contains the aortic valve and other structures. It has several components including the subcommissural triangles, aortic annulus, aortic cusps, aortic sinuses, and sinotubular junction. Each component has specific anatomical relationships within the heart. The ascending aorta begins at the aortic root and courses superiorly and to the right before the arch of the aorta gives off branches and continues posteriorly and to the left across the trachea.
preop TEE assessment of atrial septal defect is very important for making decision for device closure, properly assessed adequate rims of ASD will reduce risk of device embolization to almost nil.
there is detailed analysis of mitral valve segments by 2d transesophageal echo cardiography. There is a review on this and simplified approach how one can identify the pathological segment with great accuracy using two dimensional tee.
Our concepts of heart disease are based on the enormous reservoir of physiologic and anatomic knowledge derived from the past 70 years' of experience in the cardiac catheterization laboratory.
As Andre Cournand remarked in his Nobel lecture of December 11, 1956, the cardiac catheter was the key in the lock.
By turning this key, Cournand and his colleagues led us into a new era in the understanding of normal and disordered cardiac function in huma
preop TEE assessment of atrial septal defect is very important for making decision for device closure, properly assessed adequate rims of ASD will reduce risk of device embolization to almost nil.
there is detailed analysis of mitral valve segments by 2d transesophageal echo cardiography. There is a review on this and simplified approach how one can identify the pathological segment with great accuracy using two dimensional tee.
Our concepts of heart disease are based on the enormous reservoir of physiologic and anatomic knowledge derived from the past 70 years' of experience in the cardiac catheterization laboratory.
As Andre Cournand remarked in his Nobel lecture of December 11, 1956, the cardiac catheter was the key in the lock.
By turning this key, Cournand and his colleagues led us into a new era in the understanding of normal and disordered cardiac function in huma
Here is a detailed presentation on anatomy of heart
I sincerely agree that few of my slides are copied and most of them are prepared by myself
But that is how we help each other!!
Hope the presentation helps the one in need
And it's free to download for anyone
The whole purpose of uploading is.. So that anyone can use it ..
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Surat @ℂall @Girls ꧁❤8527049040❤꧂@ℂall @Girls Service Vip Top Model Safe
Aortic root anatomy DR NIKUNJ R SHEKHADA (MBBS,MS GEN SURG,DNB CTS SR)
1. ANATOMY OF AORTIC ROOT
BY DR NIKUNJ
(CTS RESIDENT STAR HOSPITAL)
(Coordinator:DR P.SATYENDRANATH PATHURI)
(4/7/18)
2.
3. AORTIC ROOT
• The aortic root is the anatomic segment
between the left ventricle and the
ascending aorta. It contains the aortic
valve and other anatomic elements,
which function as a unit. The aortic root
has several anatomic components:
• subcommissural triangles,
• aortic annulus,
• aortic cusps,
• aortic sinuses or sinuses of Valsalva,
• sinotubular junction.
4.
5. THE SUBCOMMISSURAL TRIANGLES
• The subcommissural triangles are
part of the left ventricular out
fow tract, but they play an
important role in the function of
the aortic valve.
• The subcommissural triangles of
the noncoronary aortic cusp are
fibrous extension of the
intervalvular brous body and
membranous septum, whereas
the subcommissural triangle
beneath the left and the right
aortic cusps is an extension of the
muscular interventricular septum.
6. THE AORTIC ANNULUS
• The aortic annulus, a fibrous structure with a scalloped shape, attaches the aortic
valve to the left ventricle.
• It is attached directly to the myocardium in approximately 45% of its
circumference, and to fibrous structures in the remaining 55%
• The diameter of the aortic annulus is 10% to 20% larger than the diameter of the
sinotubular junction of the aortic root in young patients . As the number of elastic
fibers in the arterial wall decreases with age, the sinotubular junction dilates, and
its diameter tends to become equal to that of the aortic annulus in older patients.
7. • With dilation of the aortic annulus, the subcommissural triangles of the
noncoronary cusp tend to become more obtuse as the crescent shape of the aortic
annulus along its fibrous insertion flattens.
8.
9.
10. CUSPS
• The normal aortic valve has three cusps. Each cusp has a semilunar shape and has
a base and a free margin. The base is attached to the aortic annulus in a crescent
fashion. The point at which the free margin of a cusp joins its base is the
commissure, and
• the ridge in the aortic wall that lies immediately above the commissures is the
sinotubular junction.
• The free edge of each cusp is tougher consistency than the remainder of cusp.
• At the mid point of each free edge is fibrou nodulus arantii on either side of
nodulus is extremely thin.
• The free margin of an aortic cusp extends from one of its commissures to the
other. The length of the free margin of an aortic cusp is approximately 1.5 times
the length of its base.
11. CUSPS
• The three aortic cusps often have different sizes
in a person, and the right and noncoronary cusps
are usually larger than the left cusp.
• The same cusp may have different sizes in
individuals with the same body surface area
• During diastole, the free margins and part of the
body of the three cusps touch each other
approximately in the center of the aortic root to
seal the aortic orifice.
• Thus, the average length of the free margins of
three aortic cusps must exceed the diameter of
the sinotubular junction to allow the cusps to
coapt centrally and render the aortic valve
competent .
12. • If a pathologic process causes shortening of the length of the free
margin of a cusp, or if the sinotubular junction dilates, the cusps
cannot coapt centrally, resulting in aortic insufciency .
• If the length of a free margin is elongated, the cusp prolapses, and
depending on the degree of prolapse, aortic insufficiency ensues
13. AORTIC SINUSES, OR SINUSES OF VALSALVA
• The spaces contained between the aortic
annulus and the sinotubular junction are the
aortic sinuses. There are three cusps and three
sinuses:
• left cusp and sinus,
• right cusp and sinus,
• noncoronary cusp and sinus.
• The left main coronary artery arises from the
left aortic sinus, and the right coronary artery
arises from the right aortic sinus.
• There are three sinuses of the aortic valve, each
related to the valve’s corresponding cusps. Each
sinus is divided into three areas a central part
and two adjacent parts, which are named
according to the valve cusps they adjoin.
• The noncoronary sinus is also refferred to as
the posterior aortic sinus.
14. AORTIC SINUSES, OR SINUSES OF VALSALVA
• The aortic sinuses facilitate closure of the aortic valve by creating eddies and
currents between the cusps and arterial wall .
• They also prevent the cusps from occluding the coronary artery orifices during
systole, thus guaranteeing myocardial perfusion during the entire cardiac cycle.
15.
16. RIGHT CORONARY SINUS
• entire right coronary sinus lies adjacent
to the RVOT.
• central part lies adjacent to the crista
supraventricularis,
• left part is adjacent to the area of the
RVOT in the angle between the crista
supraventricularis and the pulmonary
valve.
• posterior (noncoronary) part of the
right coronary sinus is related to the area
of the right ventricle posteroinferior to
the crista supraventricularis.
• Inferiorly, the entire right coronary sinus
is related to the interventricular septum;
the muscular septum lies under the
central and left parts, while either
membranous or muscular septum may
lie under the posterior part of the right
coronary sinus.
17. NONCORONARY SINUS
• The atrialchambers with the
intervening atrial septum lie adjacent
to the noncoronary sinus.
• right and central parts of the
noncoronary sinus are related to the
right atrium and the interatrial septum,
• left part is related to the left atrium.
• Inferiorly, the right part, like the
posterior part of the right coronary
sinus, may be related either to the
membranous or the muscular septum
depending on the size of the
membranous septum. However,
beneath the central part of the
noncoronary sinus, the membranous
septum is a constant structure. The left
part of the noncoronary sinus inserts
into the anterior mitral leaflet
18.
19. LEFT CORONARY SINUS
• posterior part of the left coronary
sinus shares the same relationship as
the left part of the noncoronary sinus,
that is, it is related to the left atrium
posteriorly and to the anterior mitral
leaflet inferiorly.
• central part of the left aortic sinus is
the only part of the aortic root that is
not related to a cardiac chamber; it is
adjacent to the epicardium only.
• right part of the left coronary sinus
lies adjacent to the pulmonary trunk
at the level of the left pulmonary
sinus. inferior to it lies the muscular
interventricular septum.
20.
21.
22. • The aortic root of young individuals is elastic and very compliant. It expands and
contracts during the cardiac cycle.
• The normal aortic root has a fairly consistent shape, and the sizes of the cusps, the
aortic annulus, the aortic sinuses, and the sinotubular junction are somewhat
interdependent.
• Thus, large cusps have a proportionally large annulus, sinus, and sinotubular
junction.
24. The ascending aorta
• The ascending aorta begins at the distal
extremity of the three aortic sinuses, the
sinotubular junction, which lies at the line
of opening of the free edge of the leaflets
of the aortic valve.
• It runs its short course passing superiorly
obliquely to the right, and slightly forward
toward the sternum. It is contained within
the fibrous pericardial sac, so its surface is
covered with serous pericardium. Its
anterior surface abuts directly on the
pulmonary trunk, which is also covered
with serous pericardium.
• the ascending aorta is related
anteromedially to the right atrial
appendage, and posterolaterally to the
right ven-tricular out flow tract and the
pulmonary trunk.
• Extrapericardially, the thymus gland lies
between it and the sternum.
25. The ascending aorta
• The medial wall of the right atrium,
the superior caval vein, and the right
pleura relate to its right side.
• On the left, its principal relationship is
with the pulmonary trunk.
26. The arch of the aorta
• The arch of the aorta begins at the
superior attachment of the pericardial
reflection just proximal to the origin of
the brachiocephalic artery
• It continues superiorly briefly before
coursing posteriorly and to the left,
crossing the lateral aspect of the distal
trachea and finally terminating on the
lateral aspect of the vertebral column.
• Here it is tethered by the parietal pleura
and the arterial ligament.
• During its course, it gives off the
brachiocephalic, the left common
carotid, and the left subclavian arteries.
•
27. • The descending, or thoracic, aorta continues
from the arch, running an initial course lateral to
the vertebral bodies and reaching an anterior
position at its termination. It gives off many
branches to the organs of the thorax throughout
its course,