- Evisceration and enucleation are surgical procedures to remove an eye. Evisceration removes the intraocular contents while leaving the outer shell intact, while enucleation removes the entire eye. Enucleation is preferred if there is suspicion of intraocular malignancy to allow for histological examination.
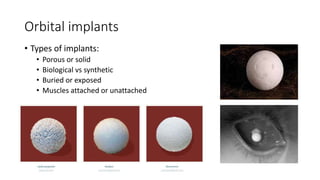
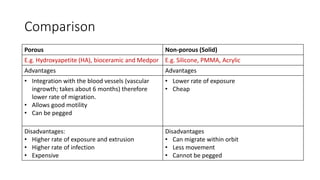
- Orbital implants are used to replace the lost volume after eye removal and allow for prosthesis motility. Implant options include porous or solid materials. Porous implants have better integration but higher risk of extrusion, while solid implants have less movement but lower extrusion risk.
- Complications after anophthalmic socket surgery can include infection, implant exposure or migration, conj












































![EYE REMOVAL TECHNIQUES [FINAL COPY BY FAITH KIMELI.] (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/eyeremovaltechniquesfinalcopybyfaithkimeli-250203210808-e559c479-thumbnail.jpg?width=640&height=640&fit=bounds)










































