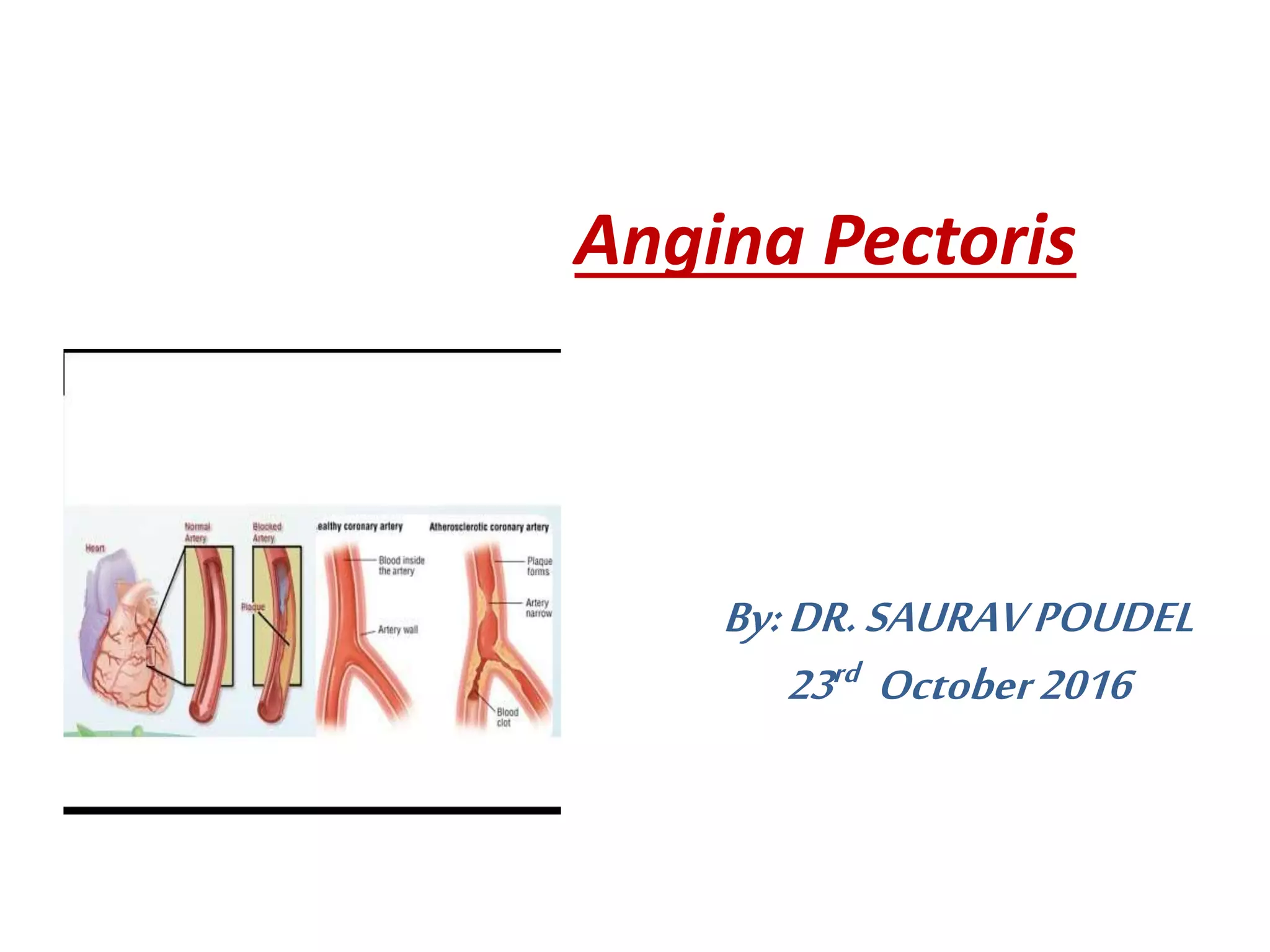
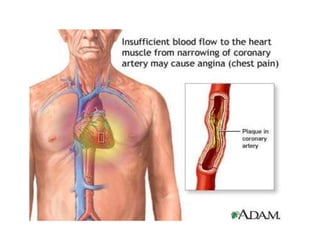
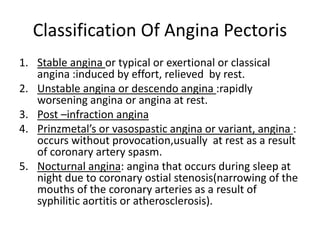
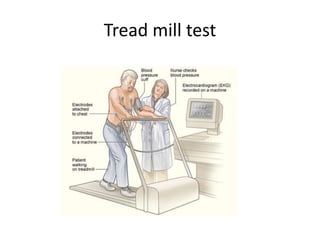
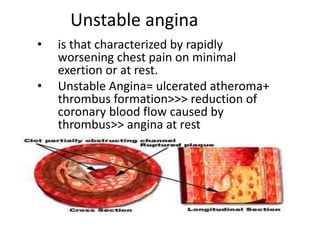
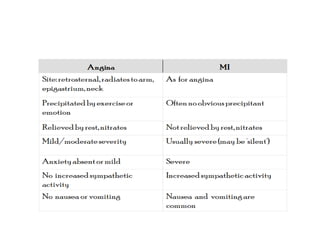
Angina pectoris is chest pain caused by an imbalance between oxygen supply and demand in the heart muscle. It is a common symptom of coronary artery disease. There are different classifications of angina including stable, unstable, and variant forms. Angina is caused by conditions that narrow the coronary arteries like atherosclerosis. Symptoms include chest pain that can radiate to the arm or jaw, brought on by exertion and relieved by rest. Diagnosis involves tests like ECG, stress testing, and angiography. Treatment focuses on lifestyle changes, medications like nitrates and beta blockers, and procedures like angioplasty if medications do not control symptoms. Unstable angina specifically involves worsening chest pain at rest and is