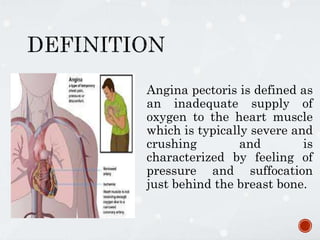
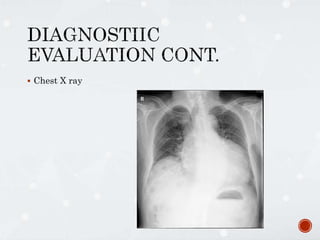
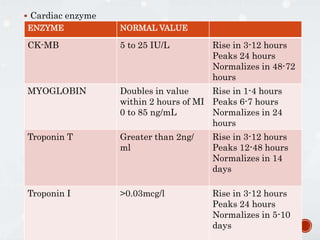
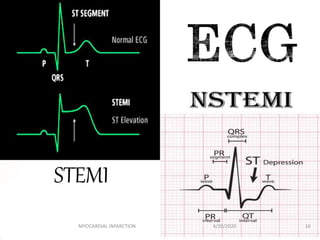
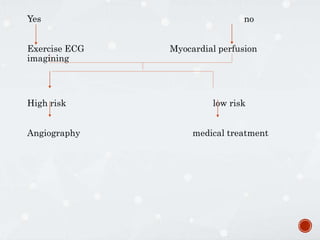
Angina pectoris is defined as chest pain due to inadequate oxygen supply to the heart muscle. It is caused by conditions that block or narrow the coronary arteries like high cholesterol or hypertension. Symptoms include chest pressure or squeezing pain that can radiate to the arms or other areas. There are different types of angina that vary in timing and triggers. Diagnosis involves health history, physical exam, ECG, cardiac enzymes and other tests. Treatment focuses on risk factor modification, medications like nitrates and calcium channel blockers, and procedures like angiography. A study found that low-dose testosterone treatment for 12 weeks in men with stable angina reduced exercise-induced ischemia and improved quality of life measures of pain and