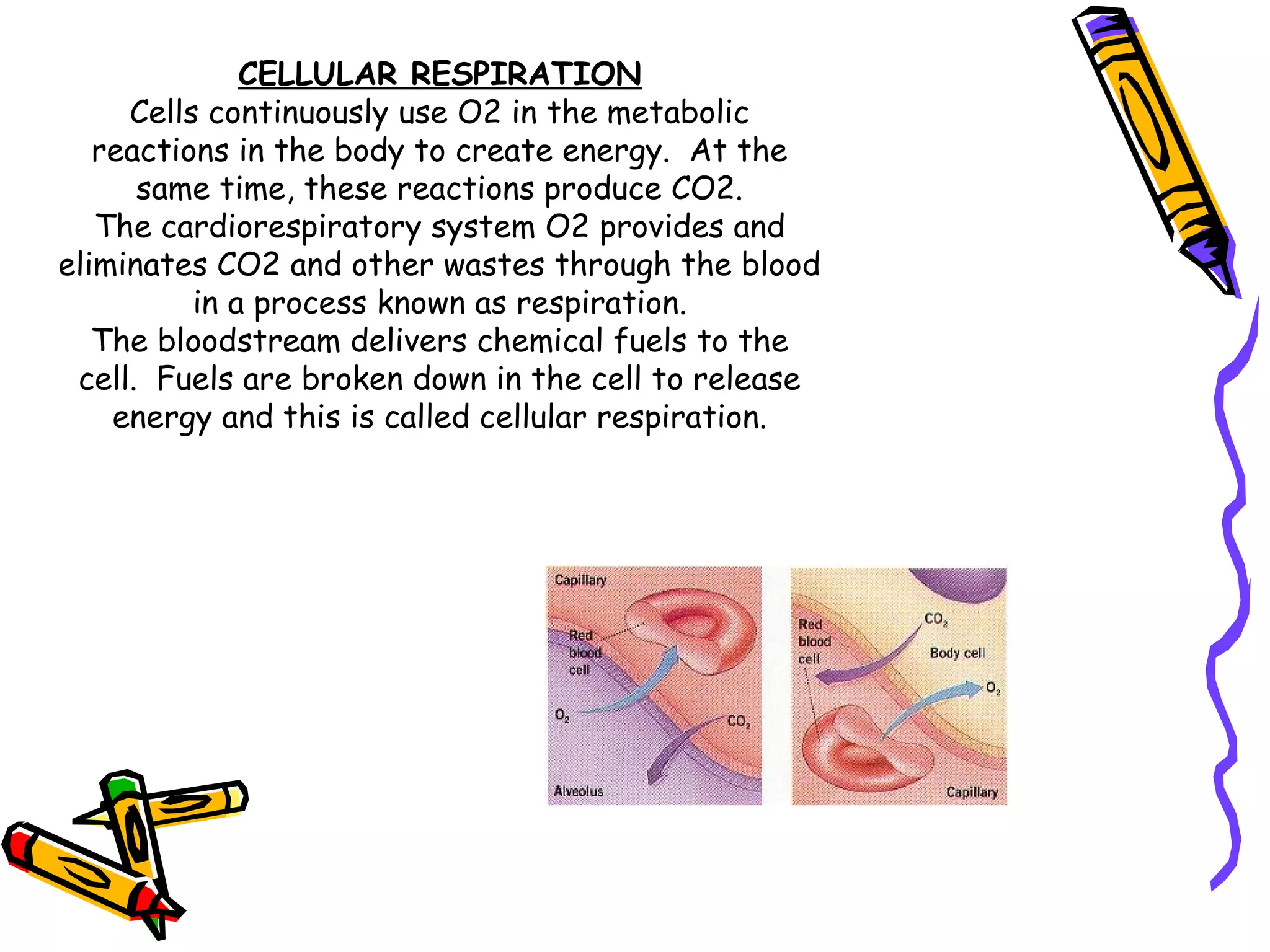
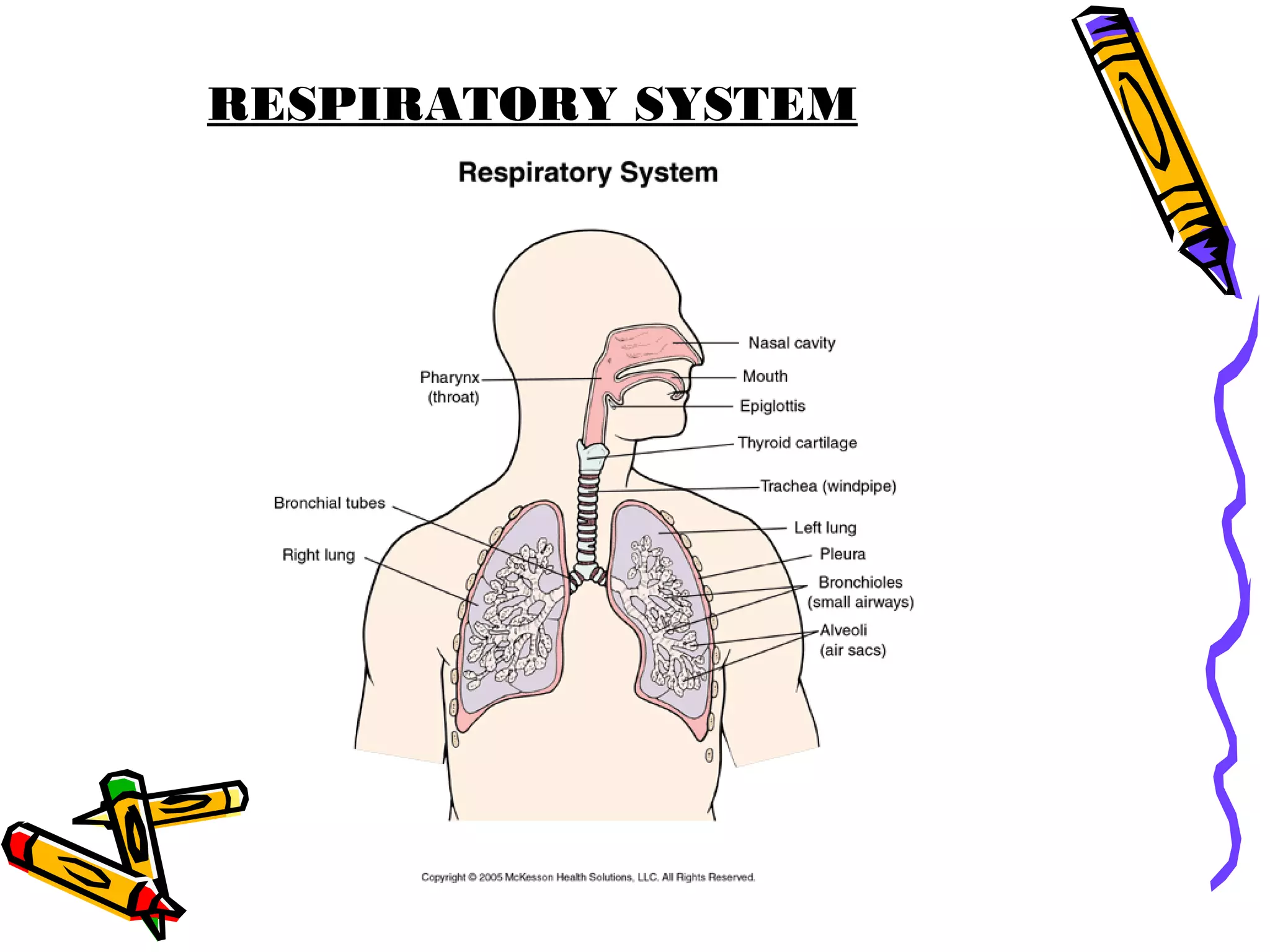
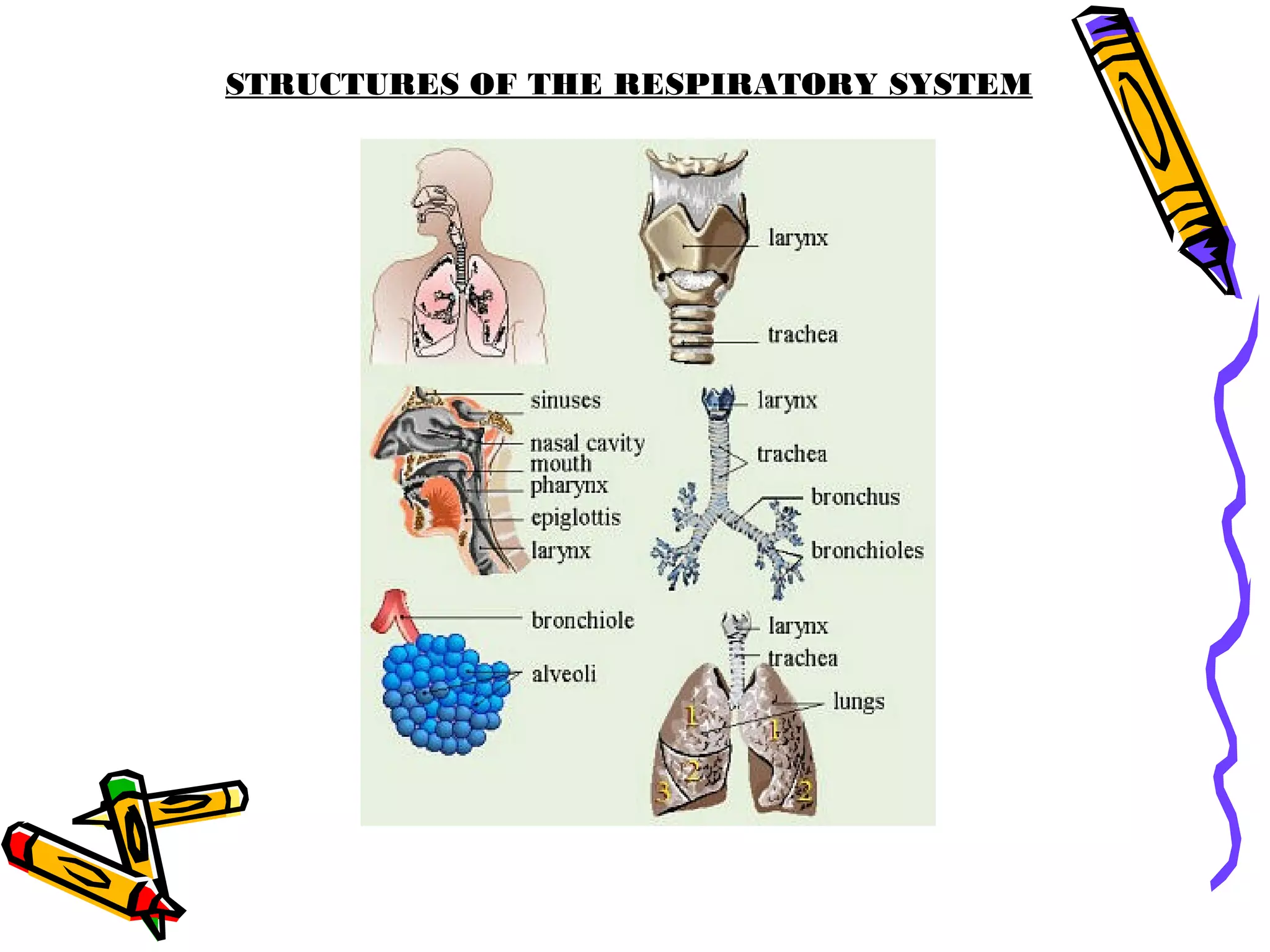
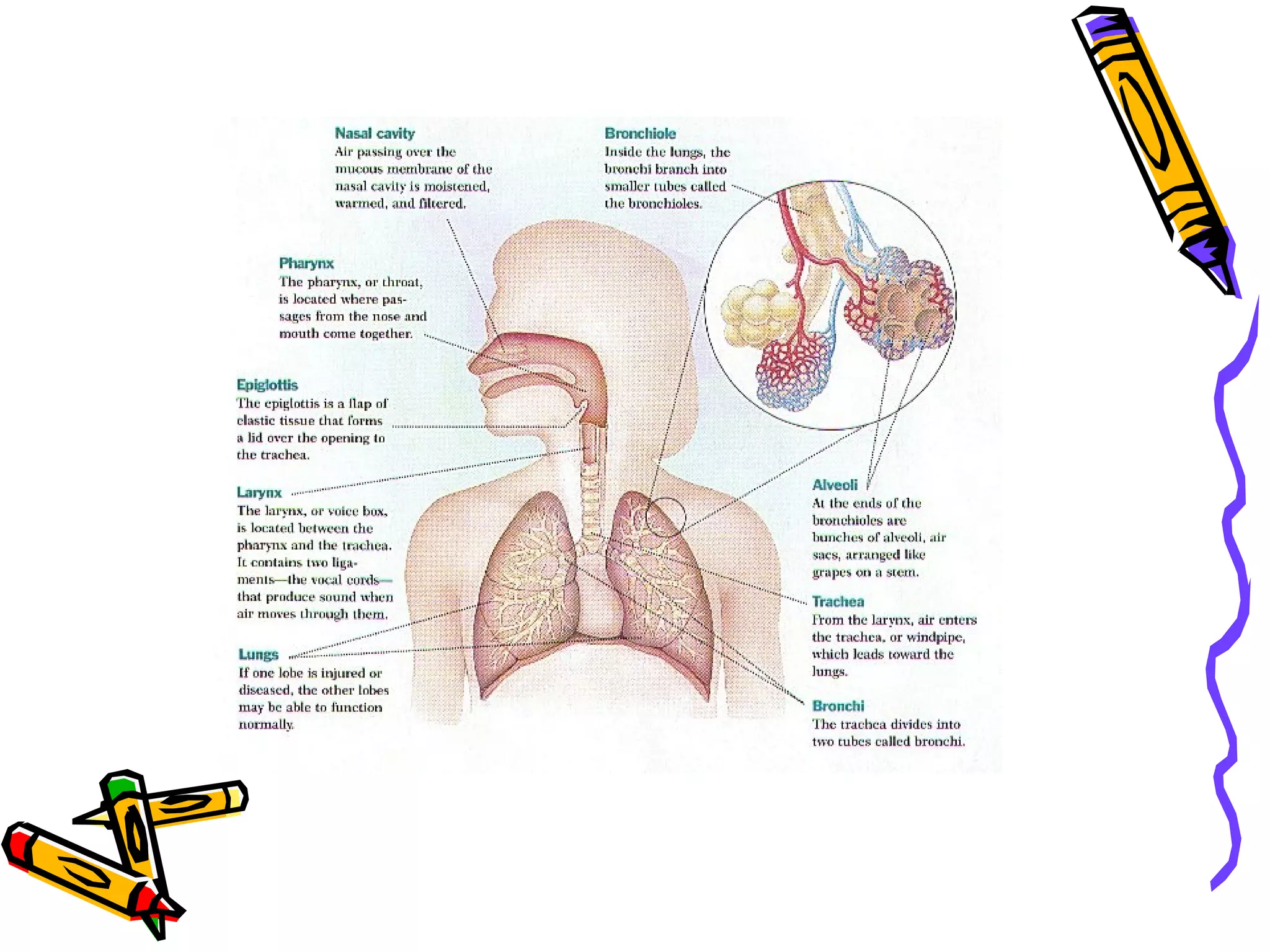
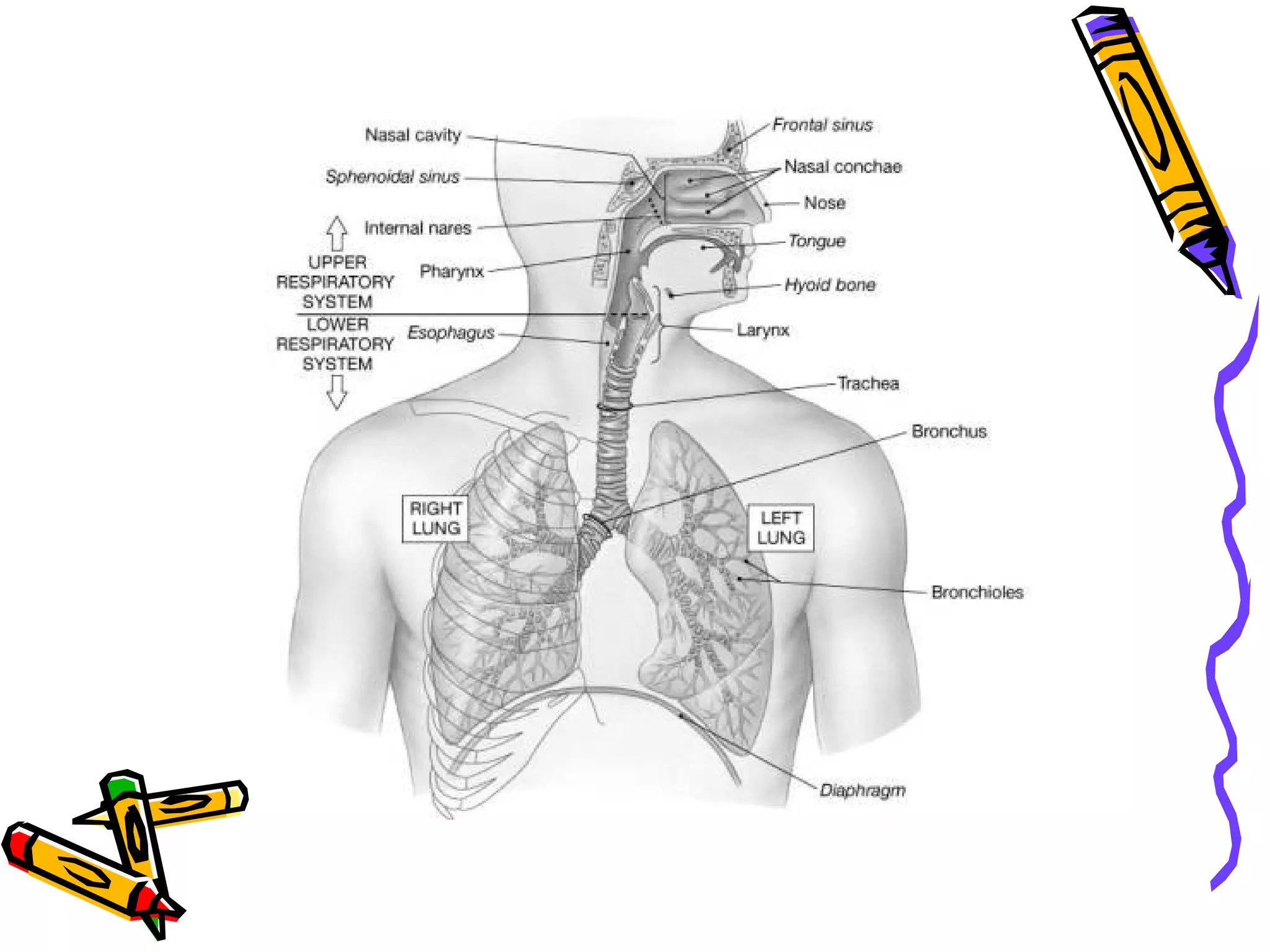
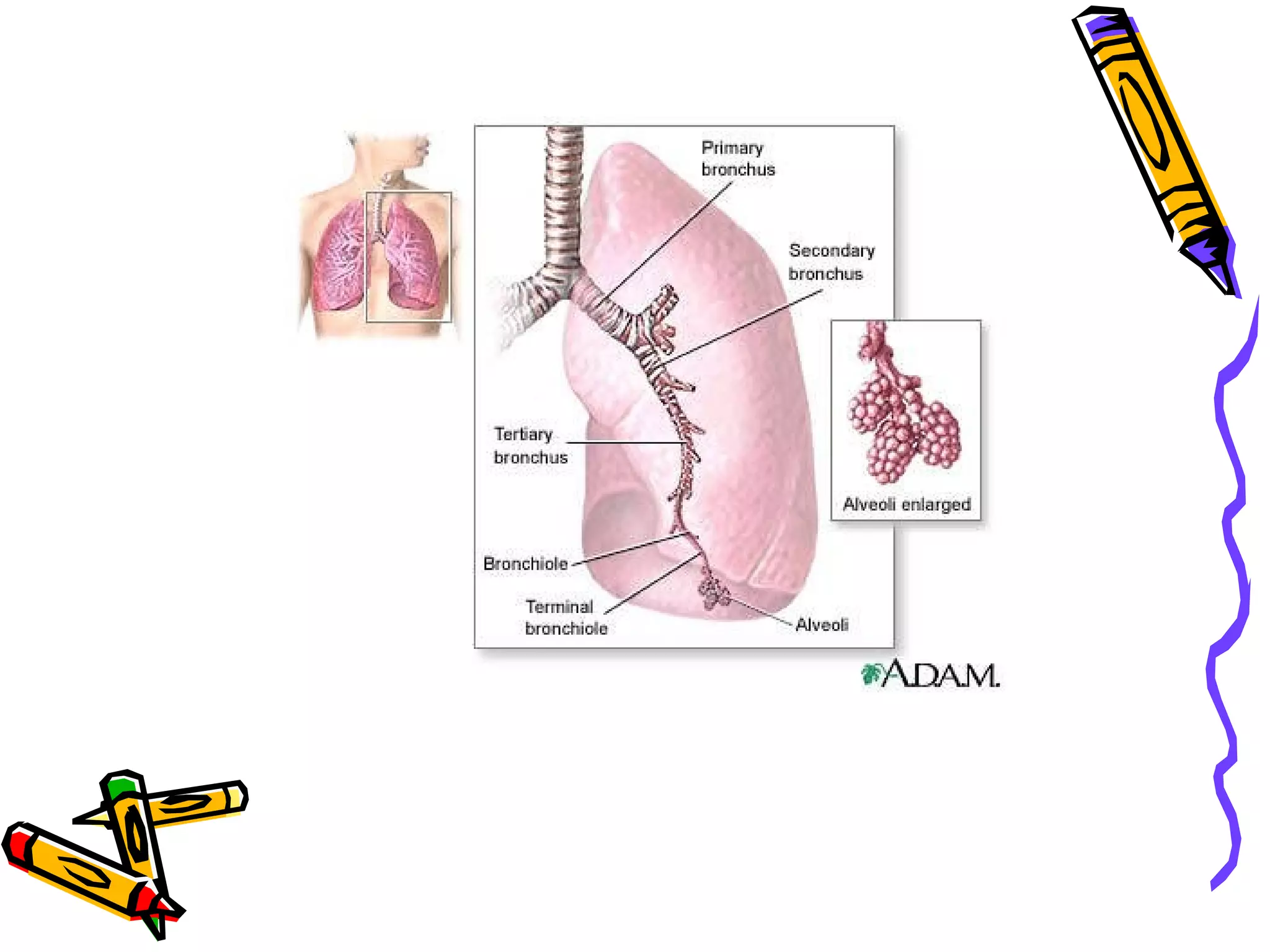
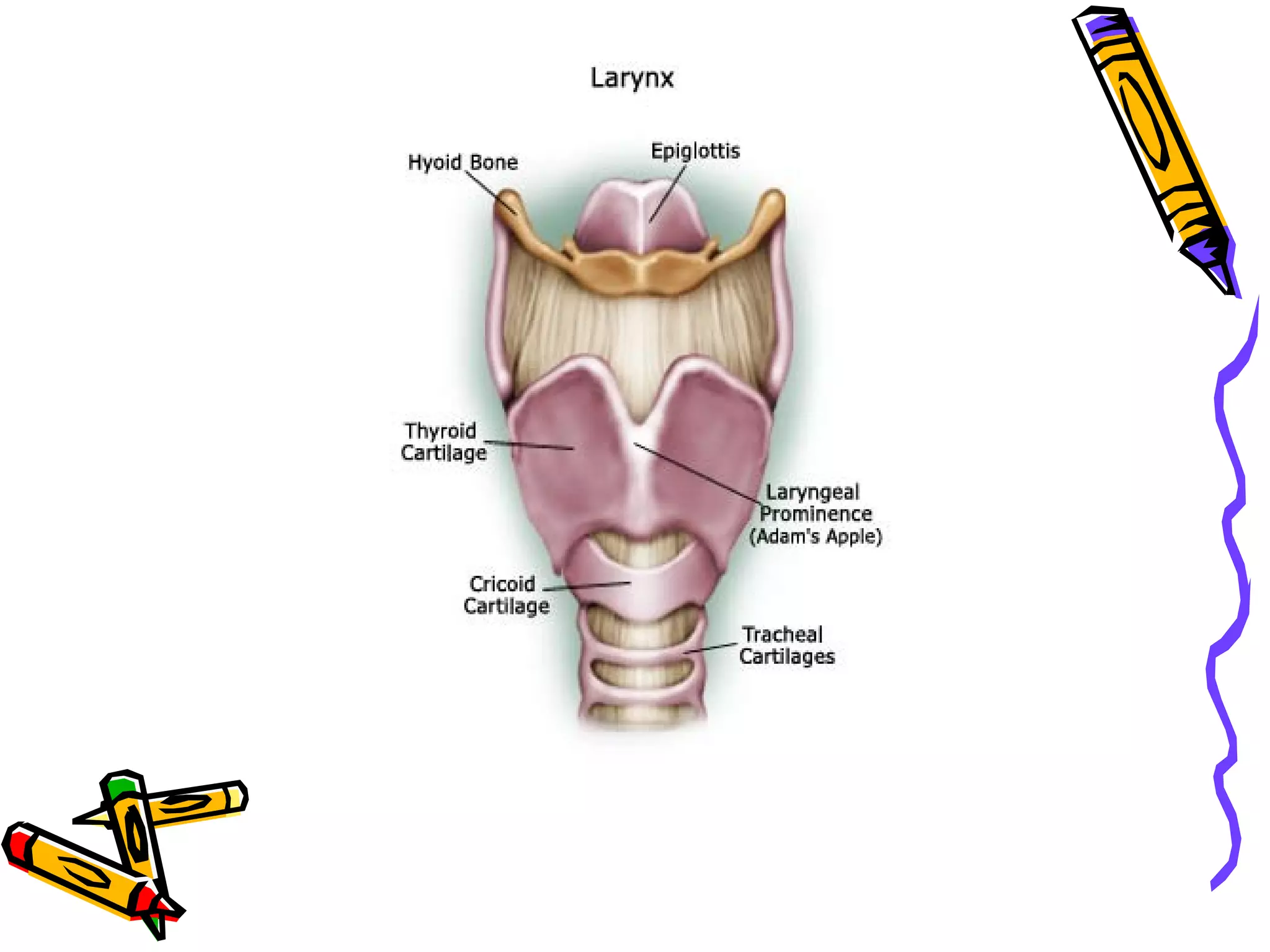
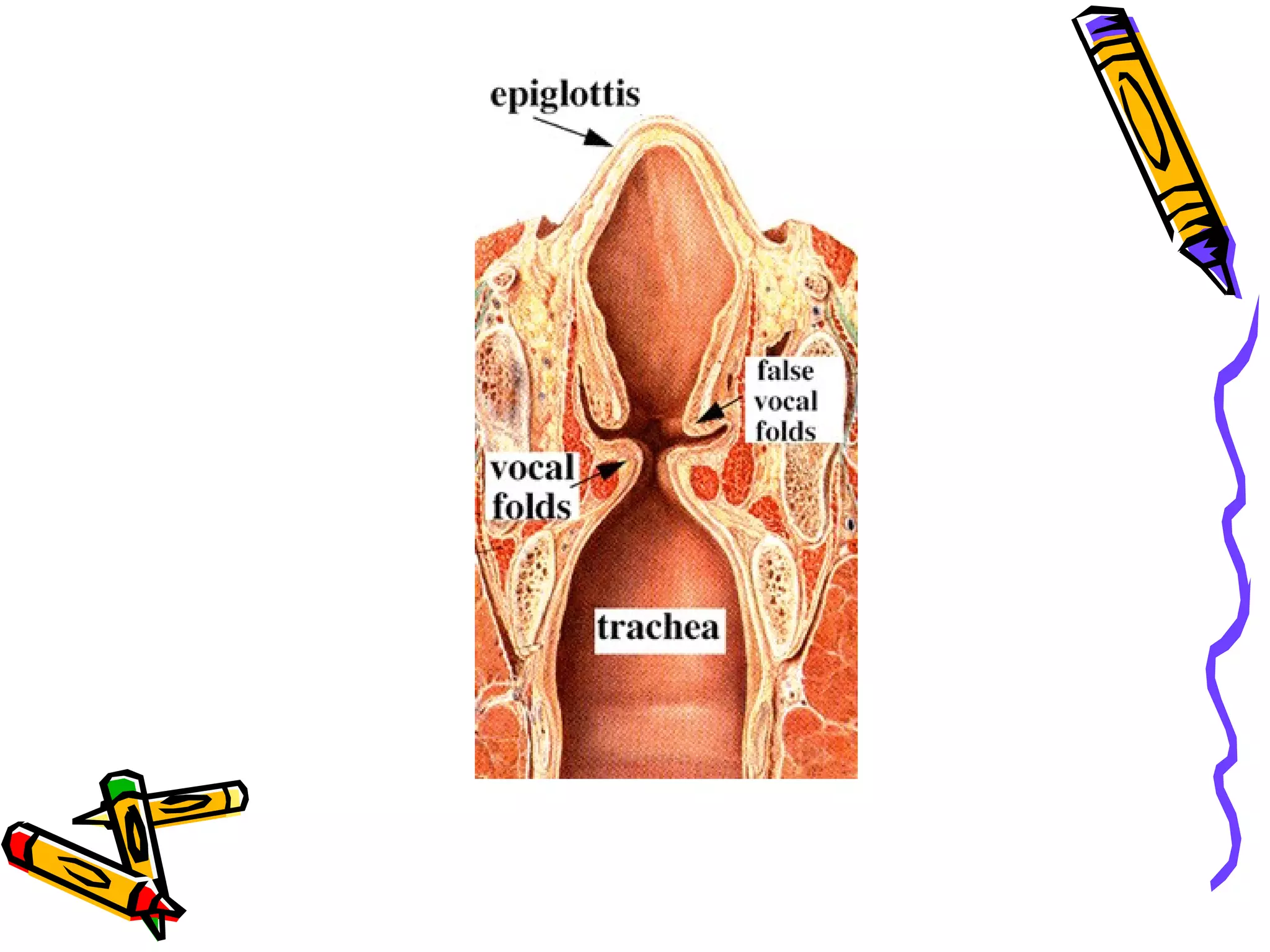
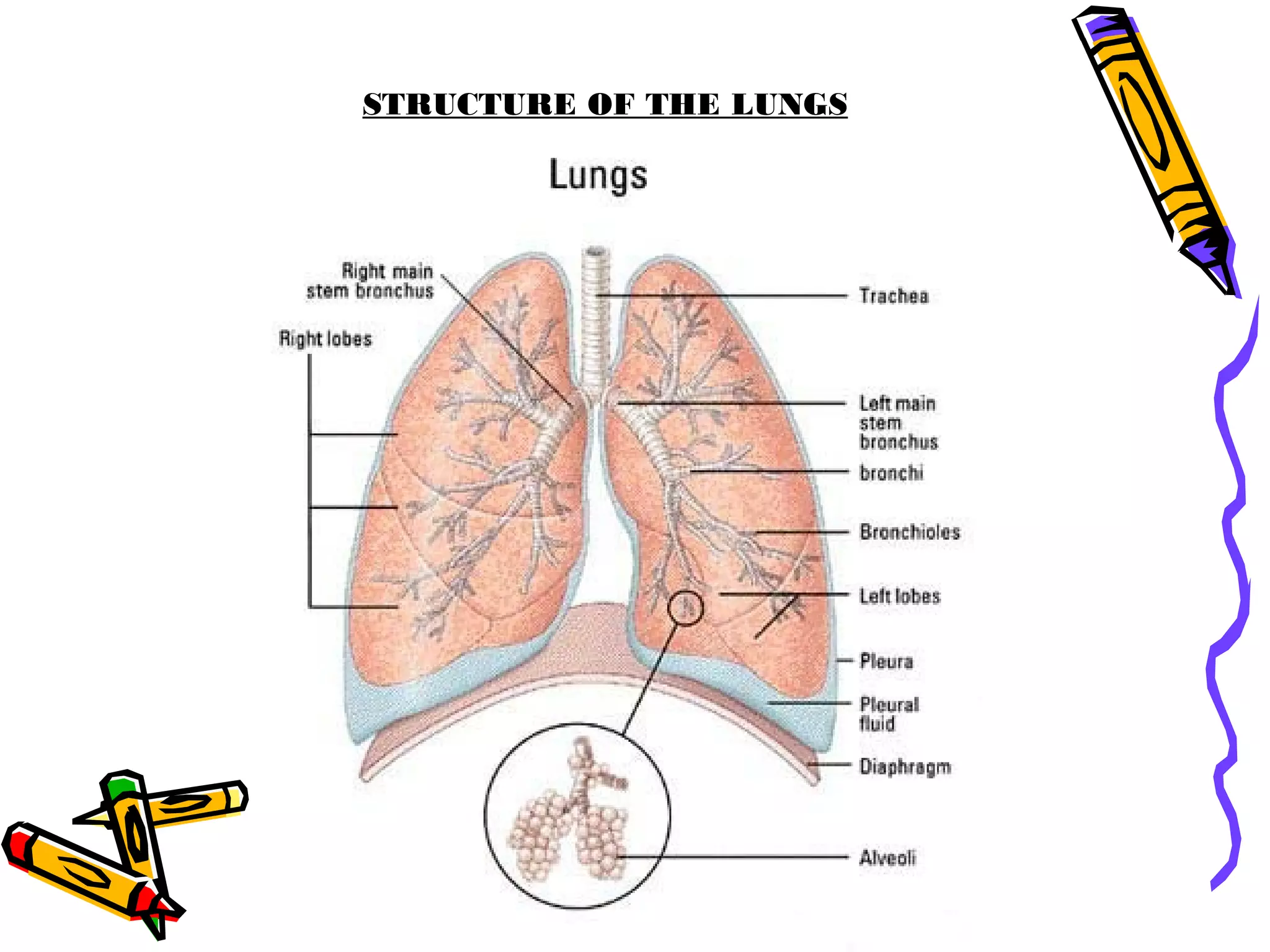
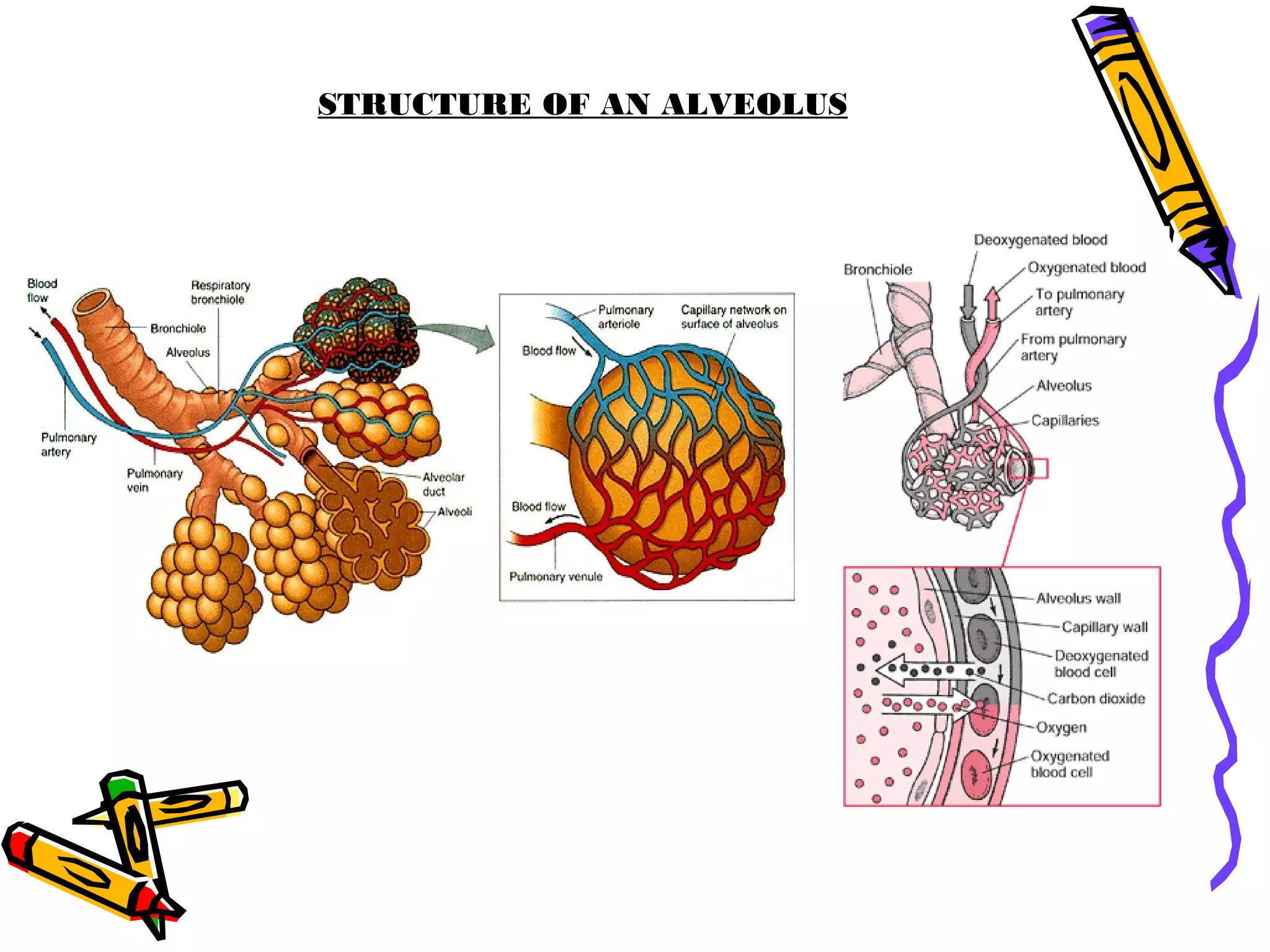
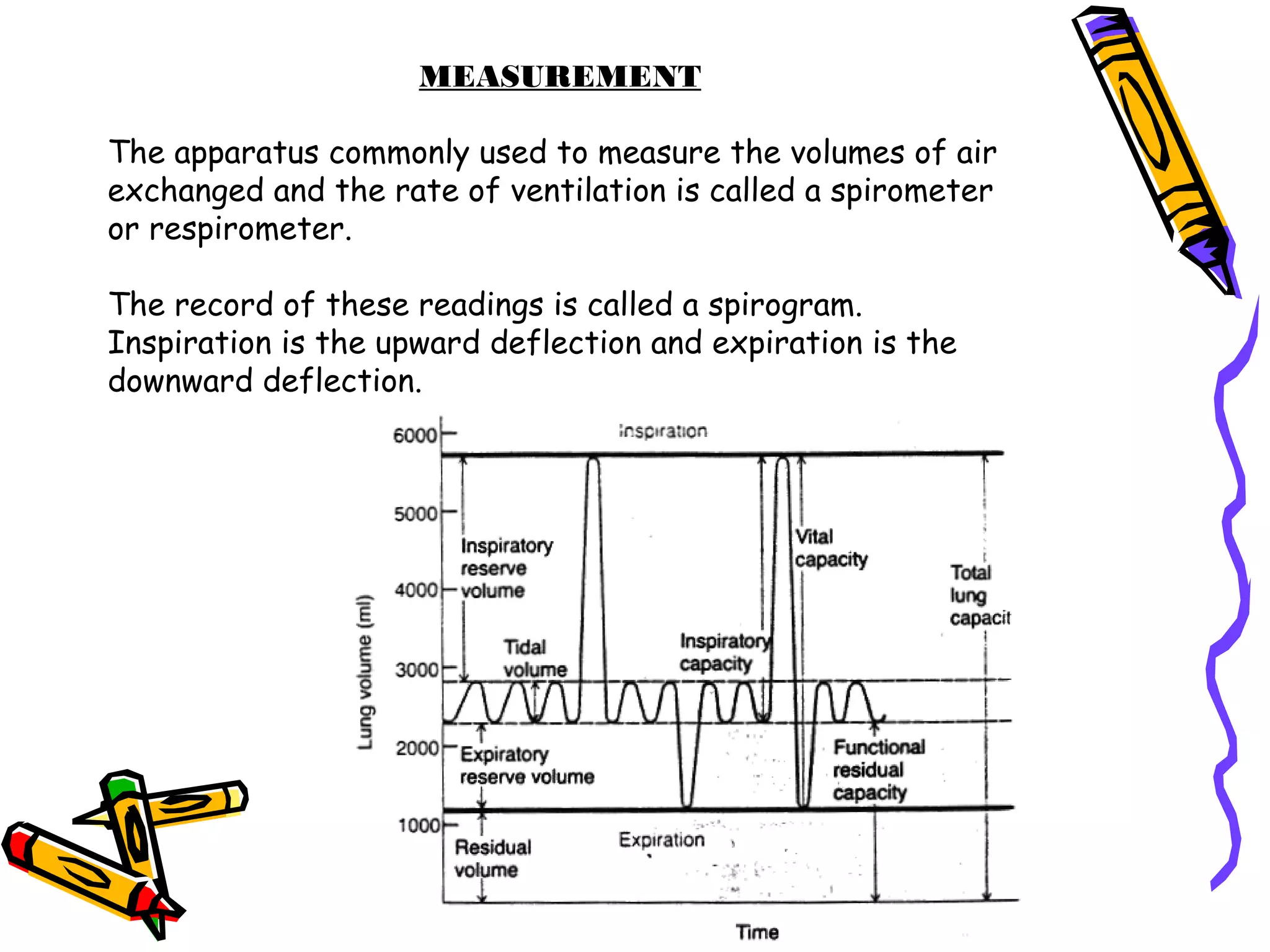
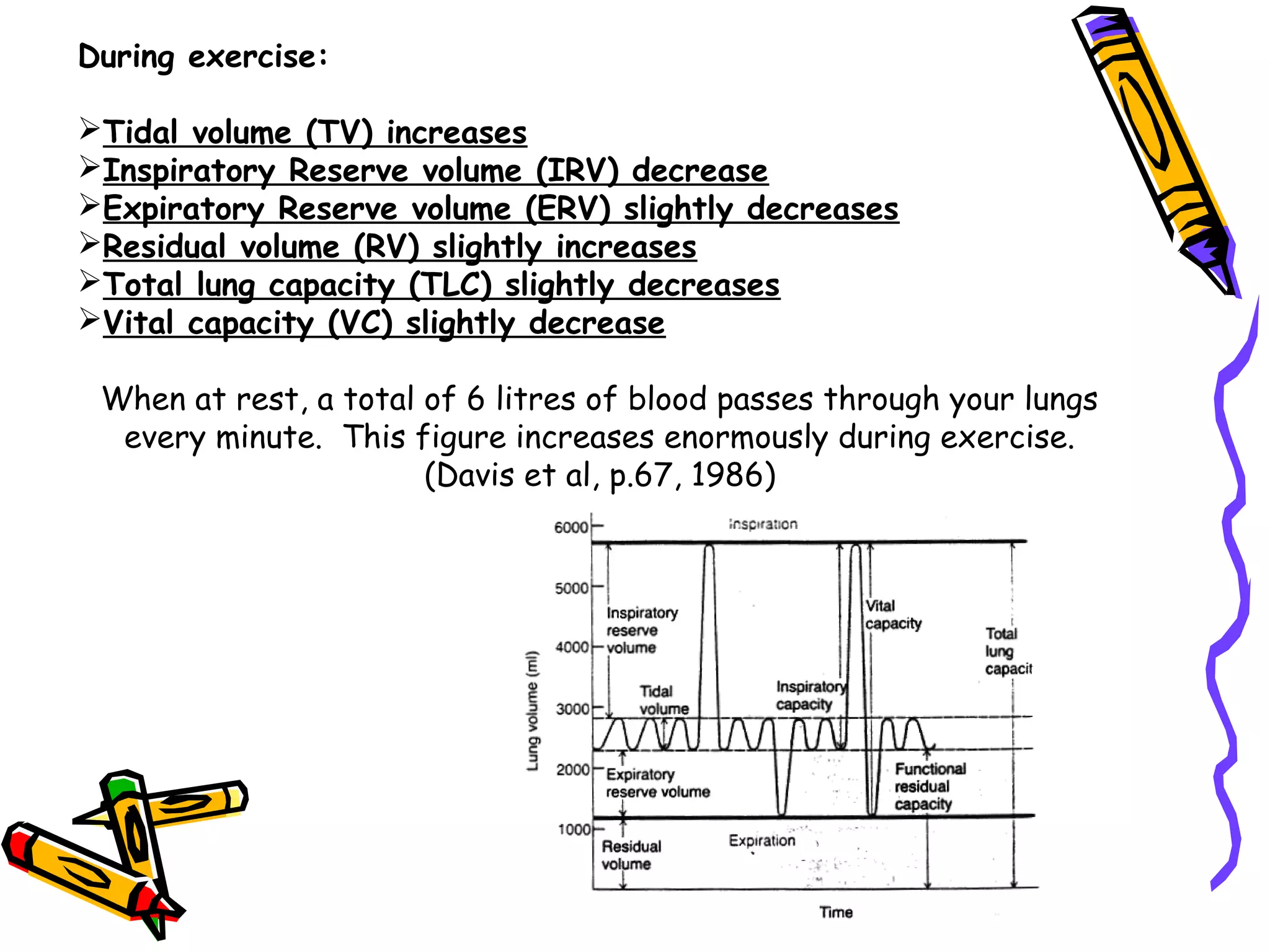
The document provides information on the structure and function of the respiratory system. It describes the major components of the respiratory system including the nasal passages, pharynx, larynx, trachea, bronchi, lungs and alveoli. It explains how oxygen and carbon dioxide are exchanged between the alveoli and blood vessels in the lungs through diffusion. The roles of inspiration and expiration in pulmonary ventilation are outlined. Adaptations to exercise such as increased ventilation and oxygen uptake are also summarized.





















![Respiratory system final [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/respiratorysystemfinalautosavedautosaved-250830120123-8e8c0dcb-thumbnail.jpg?width=640&height=640&fit=bounds)