Downloaded 507 times
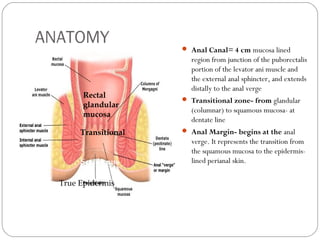
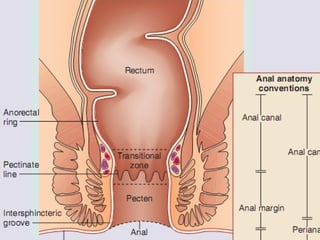
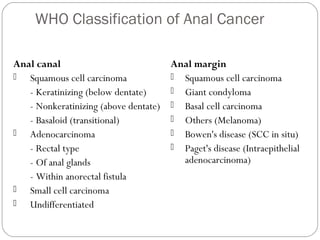
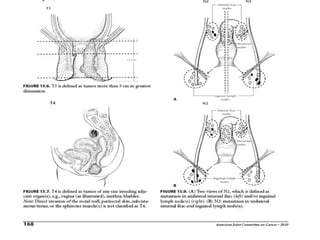
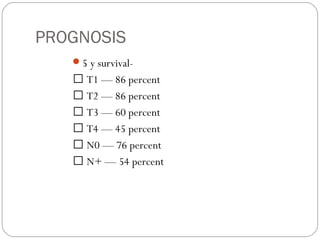
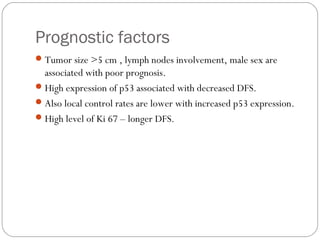


The anal canal is approximately 4 cm in length extending from the anorectal junction to the anal verge. Anal cancers are rare and mostly squamous cell carcinomas arising from the anal transitional zone. Risk factors include HPV infection and immunosuppression. Combined chemoradiotherapy is the standard first-line treatment and results in high response rates and organ preservation compared to radiation alone. Salvage surgery may be considered for select cases after failed nonsurgical treatment or as primary treatment for those who cannot tolerate chemoradiotherapy. Prognosis depends on tumor stage, with 5-year survival rates ranging from 45-86% depending on depth of invasion and nodal involvement.
















































![Chapter 39 role of radiotherapy in benign diseases.pptx [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter39roleofradiotherapyinbenigndiseases-191105205437-thumbnail.jpg?width=640&height=640&fit=bounds)






































