Downloaded 126 times



![ Anaerobic coverage is suggested to be included if there is evidence
of:
necrotizing mucositis,
sinusitis
periodontal cellulitis
perirectal cellulitis
intraabdominal infection
(including neutropenic enterocolitis [typhlitis]),
pelvic infection,
anaerobic bacteremia.](https://image.slidesharecdn.com/chapter30febrileneutropenia-191105205123/85/Chapter-30-febrile-neutropenia-22-320.jpg)

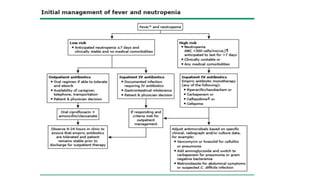

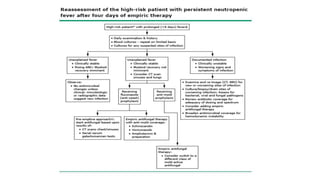


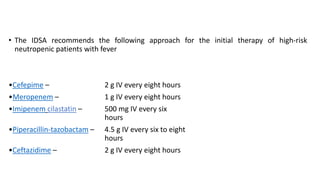
This document provides guidelines for the management of febrile neutropenia in cancer patients. It defines febrile neutropenia and outlines risks for serious infection. Initial assessment involves evaluating risk of complications to determine treatment approach. Empiric broad-spectrum antibacterial therapy should be initiated within 60 minutes of presentation to cover likely pathogens. The regimen may be modified based on infection source or persistence of fever. Early antifungal therapy should also be considered for high-risk patients.
















































![Chapter 39 role of radiotherapy in benign diseases.pptx [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter39roleofradiotherapyinbenigndiseases-191105205437-thumbnail.jpg?width=640&height=640&fit=bounds)






































