This document provides information on the management of soft tissue sarcoma. It discusses the clinical presentation, patterns of spread, imaging, histology, grading, staging, prognostic factors and management of soft tissue sarcomas. The key points are:
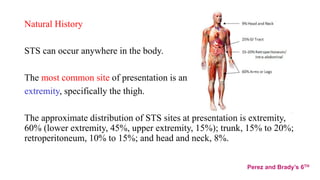
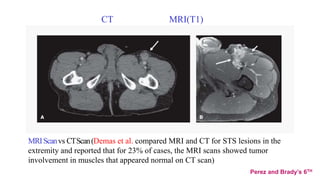
1) Soft tissue sarcomas most commonly present as painless swellings in the extremities and can invade locally along fascial planes. Imaging like MRI is important for assessing tumor extent.
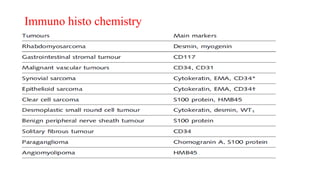
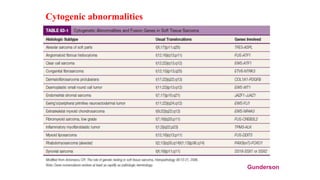
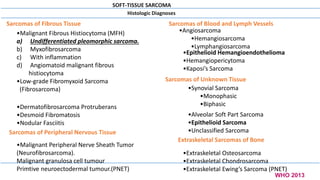
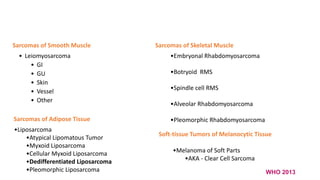
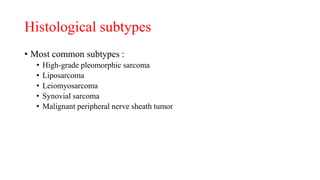
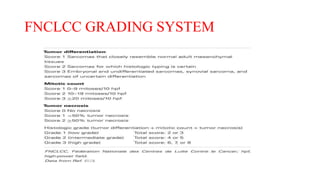
2) Histologically, the most common subtypes are undifferentiated pleomorphic sarcoma and liposarcoma. Grading systems consider tumor differentiation, mitosis and necrosis.
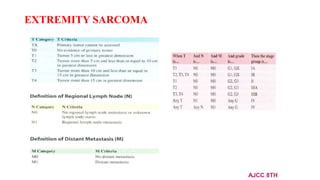
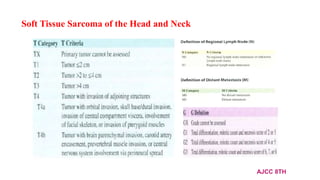
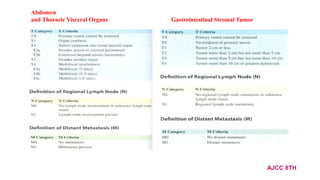
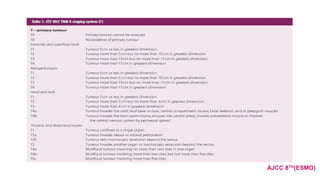
3) Staging is based on tumor size, depth, nodal status and metastasis
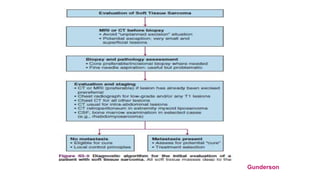
![Investigation:
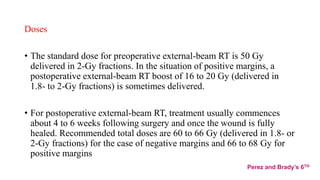
• Following appropriate imaging assessment, the standard approach to
diagnosis consists of multiple core needle biopsies.
• However, an excisional biopsy may be the most practical option for < 3 cm
superficial lesions.
( Excisional biopsy should be avoided, especially for lesions >3 cm in size, as the contamination of
surrounding tissue planes may require the definitive resection to be more extensive.)-DEVITA
• An open biopsy may be another option in selected cases.
• A biopsy may underestimate the tumor malignancy grade. Therefore, when
preoperative treatment is an option, radiological imaging [PET] may be
useful, in addition to pathology, in providing the clinician with information
that helps to estimate the malignancy grade
ESMO-2018](https://image.slidesharecdn.com/softtissuesarcoma-210821055132/85/Soft-tissue-sarcoma-10-320.jpg)
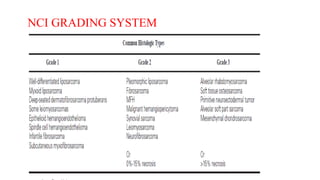
![Grading
• Under histological grading , the two most important criteria appear to be the mitotic
index and the extent of tumor necrosis.
• The two systems most favoured by pathologists are those designated as
the French Federation of Cancer Centres Sarcoma Group (FNCLCC)
[tumour differentiation , mitotic count and necrosis]
The National Cancer Institute (NCI)
[tumor histology and amount of tumor necrosis ]](https://image.slidesharecdn.com/softtissuesarcoma-210821055132/85/Soft-tissue-sarcoma-19-320.jpg)




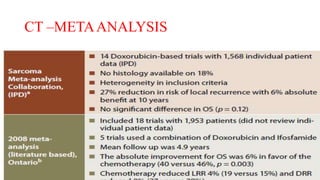
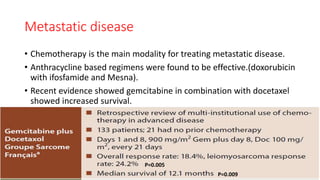
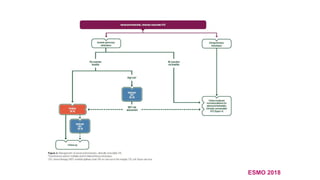
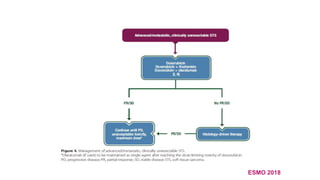
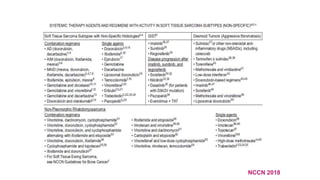
![Management of advanced/metastatic disease
• Metachronous (disease-free interval1 year), resectable lung metastases without extrapulmonary
disease are managed with surgery as standard treatment, if complete excision of all lesions is feasible.
• Standard ChT is based on anthracyclines as the first-line treatment [I, A]. Multi-agent ChT with
adequate-dose anthracyclines plus ifosfamide may be the treatment of choice, particularly in subtypes
sensitive to ifosfamide, when a tumour response is felt to be potentially advantageous and patient PS
is good [I, B]
• The combination of doxorubicin with an anti-PDGFRA agent, olaratumab, is option.
• Gemcitabine/docetaxel combination is not generally recommended as a first-line therapy for
advanced STS patients [I, D]
• Imatinib is standard medical therapy for those rare patients with dermatofibrosarcoma protuberans.
• Trabectedin is an option for second line and is approved for advanced previously treated STS.
• Pazopanib is an option in non-adipogenic STS.
• Eribulin is an option in patients with liposarcomas and LMS.
• Regorafenib is an option in doxorubicin-pretreated advanced, non-adipogenic STS patients.
• Crizotinib in inflammatory myofibroblastic tumours associated with ALK translocations.
Sunitinib and cediranib in alveolar soft part sarcoma, where the molecular target is as yet unclear and
Sunitinib in solitary fibrous tumours [IV, C]
ESMO 2018](https://image.slidesharecdn.com/softtissuesarcoma-210821055132/85/Soft-tissue-sarcoma-66-320.jpg)