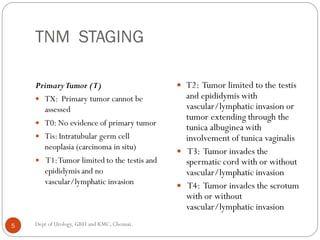
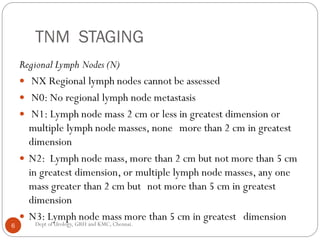
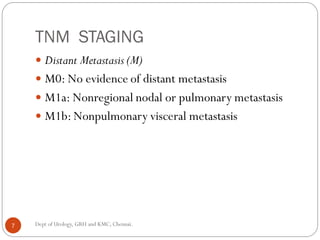
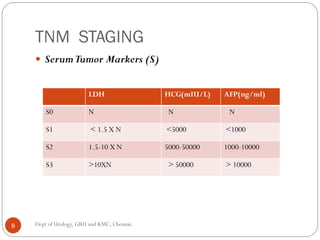
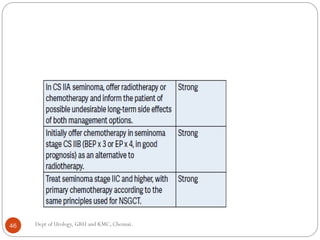
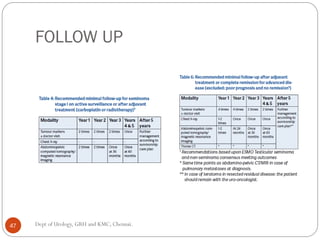
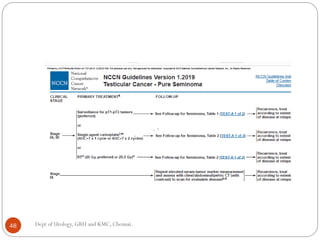
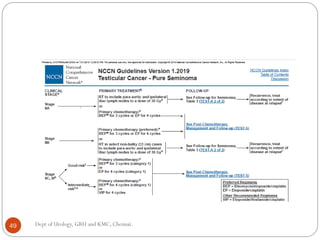
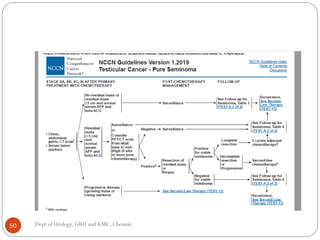
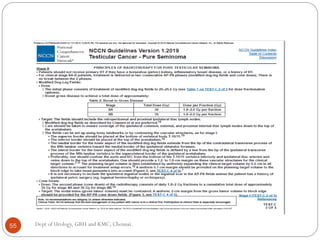
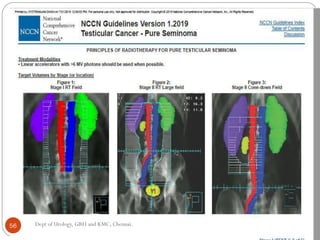
This document discusses the management of seminoma testis. It provides information on staging, pathology, treatment approaches including radical orchidectomy, surveillance, radiotherapy and chemotherapy for different stages of seminoma. For stage I seminoma, options discussed are surveillance, radiotherapy and primary chemotherapy. For advanced stages, cisplatin-based chemotherapy is the standard treatment. Approaches to residual masses after chemotherapy and relapse are also summarized. The document aims to provide guidance on achieving cure for seminoma with minimal morbidity through appropriate treatment based on stage.

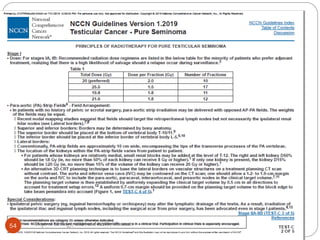
![Stage I Seminoma
Primary chemotherapy
A single agent course of
carboplatin
Low myelotoxicity and
gonadal toxicity
Recurrence rate 9%.
Primary chemotherapy
Two courses of carboplatin
were associated with no
relapses .
The optimal dosing of
carboplatin is calculated by
the formula 7 ×
(glomerular filtration rate
[GFR, mL/min] + 25) mg
23 Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/testis-carcinoma-management-seminoma-210610131155/85/Testis-carcinoma-management-seminoma-23-320.jpg)













































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










