Downloaded 49 times









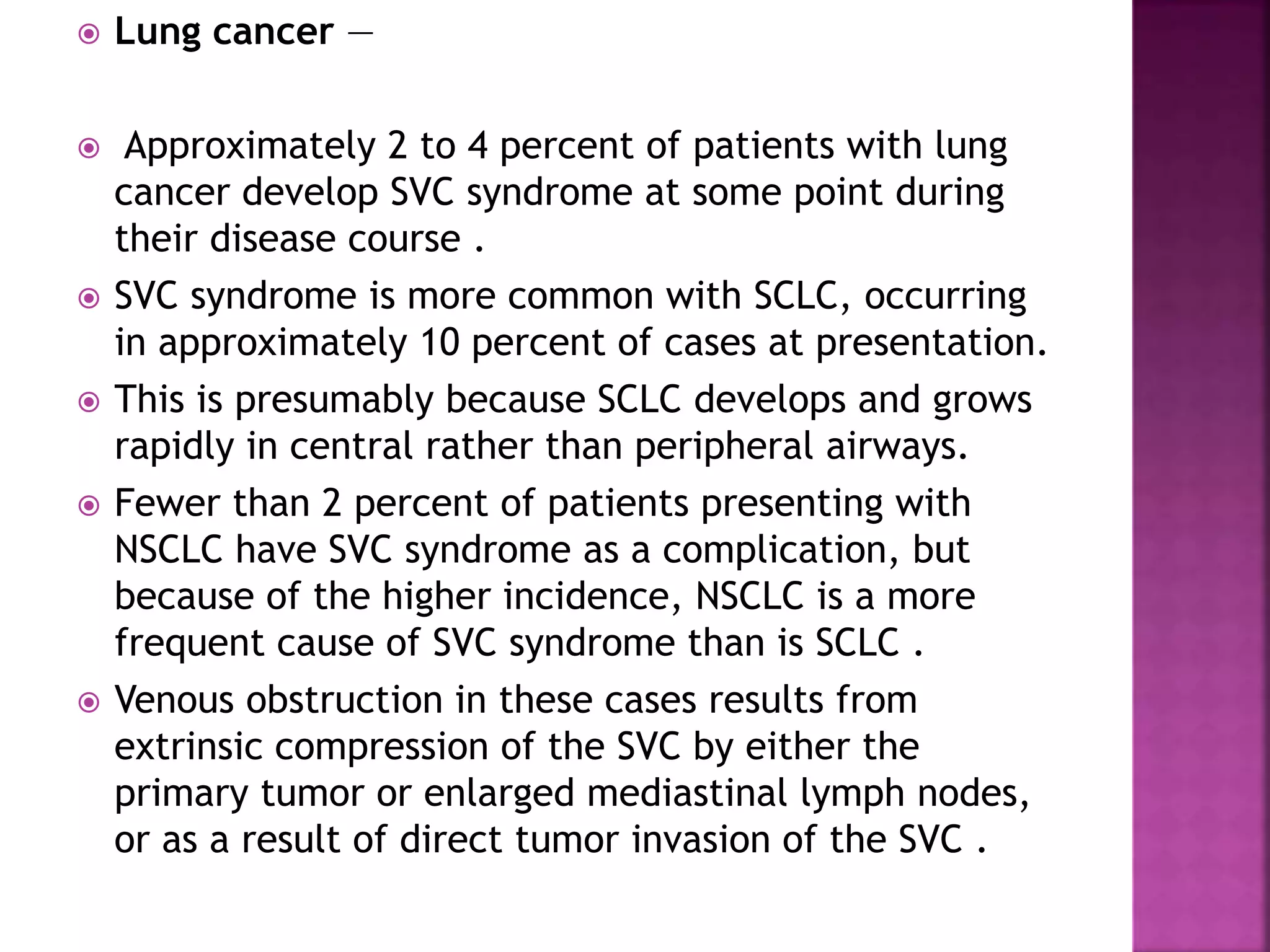




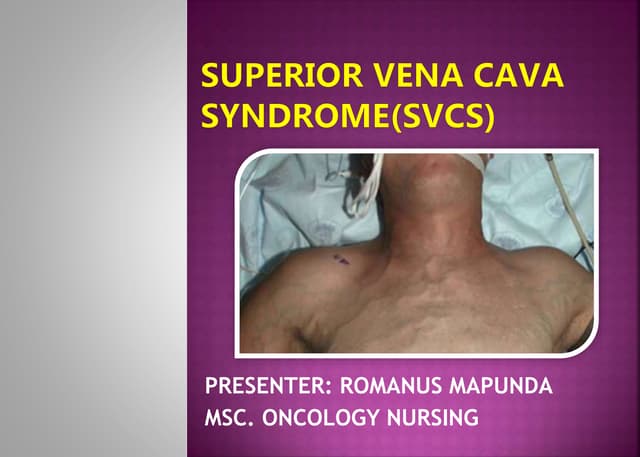
Superior vena cava (SVC) syndrome results from obstruction of blood flow through the SVC, which can be caused by external compression or invasion by adjacent tumors or thrombosis within the SVC. The most common causes are lung cancer, lymphoma, and thrombosis related to intravenous devices. Obstruction of the SVC increases venous blood pressure as collateral veins form, potentially causing symptoms like head and neck swelling, dyspnea, and cough. SVC syndrome is diagnosed based on symptoms and imaging evidence of SVC obstruction.















































![Chapter 39 role of radiotherapy in benign diseases.pptx [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter39roleofradiotherapyinbenigndiseases-191105205437-thumbnail.jpg?width=640&height=640&fit=bounds)





































