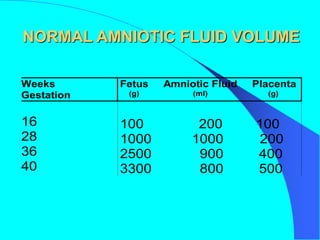
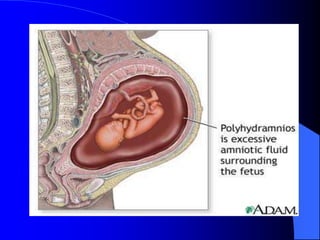
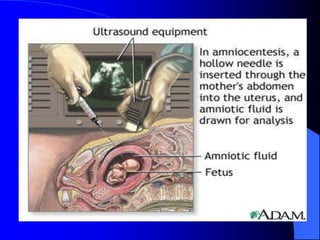
This document discusses amniotic fluid volume during pregnancy. It defines polyhydramnios as over 2000cc of amniotic fluid and provides potential causes such as fetal anomalies, diabetes, and multiples. Symptoms in the mother include dyspnea and abdominal pain. Diagnosis is made through ultrasound. Oligohydramnios is defined as under 5cc and can be caused by postdates, fetal anomalies, or restricted growth. It carries risks of fetal malformations and respiratory issues at birth.












































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



