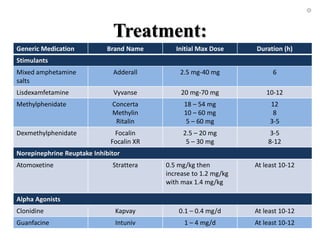
Attention-deficit/hyperactivity disorder (ADHD) is a neurobehavioral disorder defined by inattention, hyperactivity, and impulsivity. It has genetic and environmental causes and affects the dopaminergic and noradrenergic neurotransmitter systems in the brain. ADHD is diagnosed clinically based on the number of symptoms present over several months in multiple environments for children or adolescents. The primary treatment is stimulant medication, though nonstimulants may also be used. Left untreated, ADHD can lead to academic underachievement, low self-esteem, interpersonal issues, and higher risk behaviors as an adolescent.
















































![ADHD (best)]](https://cdn.slidesharecdn.com/ss_thumbnails/bykhaihojoshuagabriel1-1234763718979961-1-thumbnail.jpg?width=640&height=640&fit=bounds)























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







