Downloaded 137 times
![ Autism’s environmental risk
factors
• Increased risk
• Advanced parent age (either parent)
• Pregnancy and birth complications
(e.g. extreme prematurity [before 26
weeks], low birth weight, multiple
pregnancies [twin, triplet, etc.])
• Pregnancies spaced less than one
year apart
• Decreased risk
Prenatal vitamins containing folic acid,
before and at conception and through
pregnancy
• No effect on risk
Vaccines. The results of this research is
clear that Vaccines do not cause autism.
The American Academy of Pediatrics has
compiled a comprehensive list of this
research.
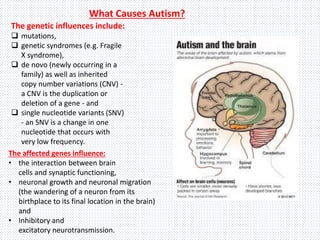
Autism’s genetic risk factors
• Changes in certain genes increase the
risk that a child will develop autism.
• If a parent carries one or more of these
gene changes, they may get passed to a
child (even if the parent does not have
autism).
• Other times, these genetic changes
arise spontaneously in an early embryo
or the sperm and/or egg that combine
to create the embryo.
• Again, the majority of these gene
changes do not cause autism by
themselves.](https://image.slidesharecdn.com/vari1-181115143100/85/autism-spectrum-disorder-a-general-introduction-14-320.jpg)


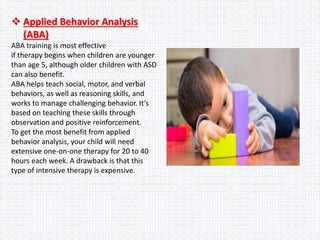
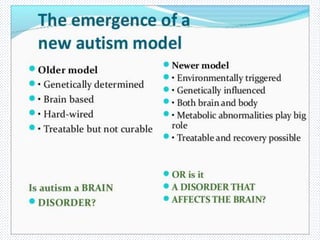
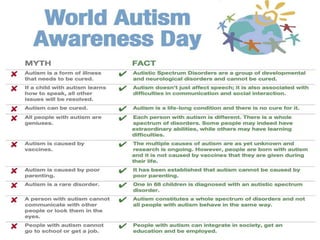

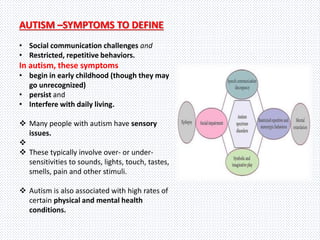
Autism spectrum disorder (ASD) is a developmental disorder characterized by challenges with social skills, repetitive behaviors, speech and nonverbal communication. The causes are both genetic and environmental. Symptoms begin in early childhood and can range from mild to severe. Treatment focuses on education, behavioral therapies, medication management and developing communication and life skills.









































![Autism[2]](https://cdn.slidesharecdn.com/ss_thumbnails/autism2-100901200334-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)













































