This document provides information on the assessment and treatment of ADHD across the lifespan. It begins with multiple choice questions related to ADHD diagnosis and treatment. It then covers topics like the diagnostic criteria for ADHD according to the DSM-IV-TR, common co-morbidities, neurobiology, treatment guidelines, and medication options. Psychoeducation and classroom interventions are also discussed as important components of treatment. Legal rights and services students are entitled to under laws like IDEA are reviewed. Throughout, the document emphasizes the clinical nature of ADHD and importance of properly diagnosing and treating the disorder.






![13
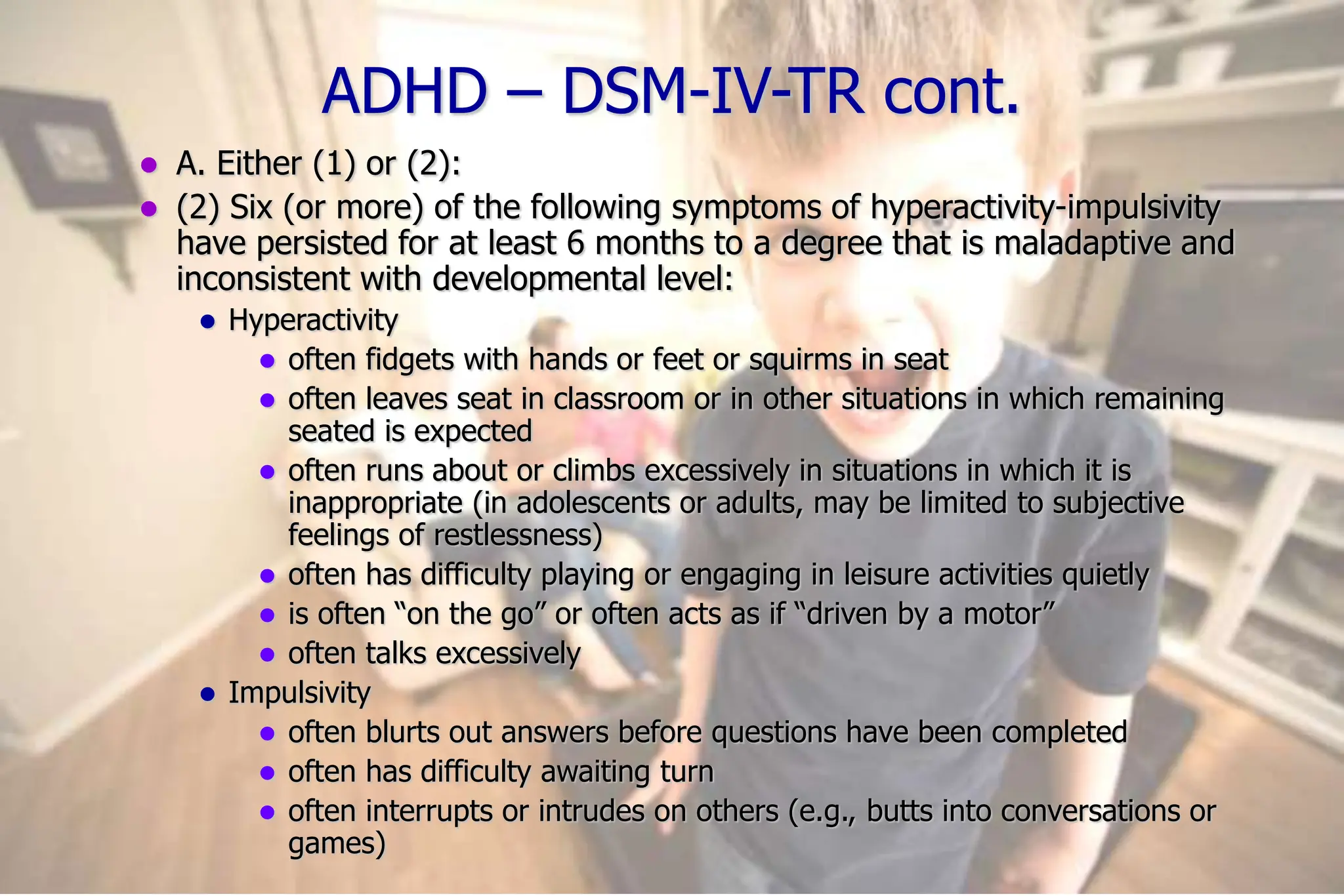
ADHD – DSM-IV-TR cont.
B. Some hyperactive-impulsive or inattentive symptoms that caused
impairment were present before age 7 years.
C. Some impairment from the symptoms is present in two or more
settings (e.g., at school [or work] and at home).
D. There must be clear evidence of clinically significant impairment in
social, academic, or occupational functioning.
E. The symptoms do not occur exclusively during the course of a
pervasive developmental disorder, schizophrenia, or other psychotic
disorder and are not better accounted for by another mental disorder
(e.g., mood disorder, anxiety disorder, dissociative disorder, or a
personality disorder).
Code based on type:
Attention-deficit/hyperactivity disorder, combined type: if both Criteria A1 and
A2 are met for the past 6 months
Attention-deficit/hyperactivity disorder, predominantly inattentive type: if
Criterion A1 is met but Criterion A2 is not met for the past 6 months
Attention-deficit/hyperactivity disorder, predominantly hyperactive-impulsive
type: if Criterion A2 is met but Criterion A1 is not met for the past 6 months](https://image.slidesharecdn.com/adhdacrossthelifespan-240120164356-ed34cf68/75/ADHD-Across-the-Lifespan-ppt-13-2048.jpg)

















![39
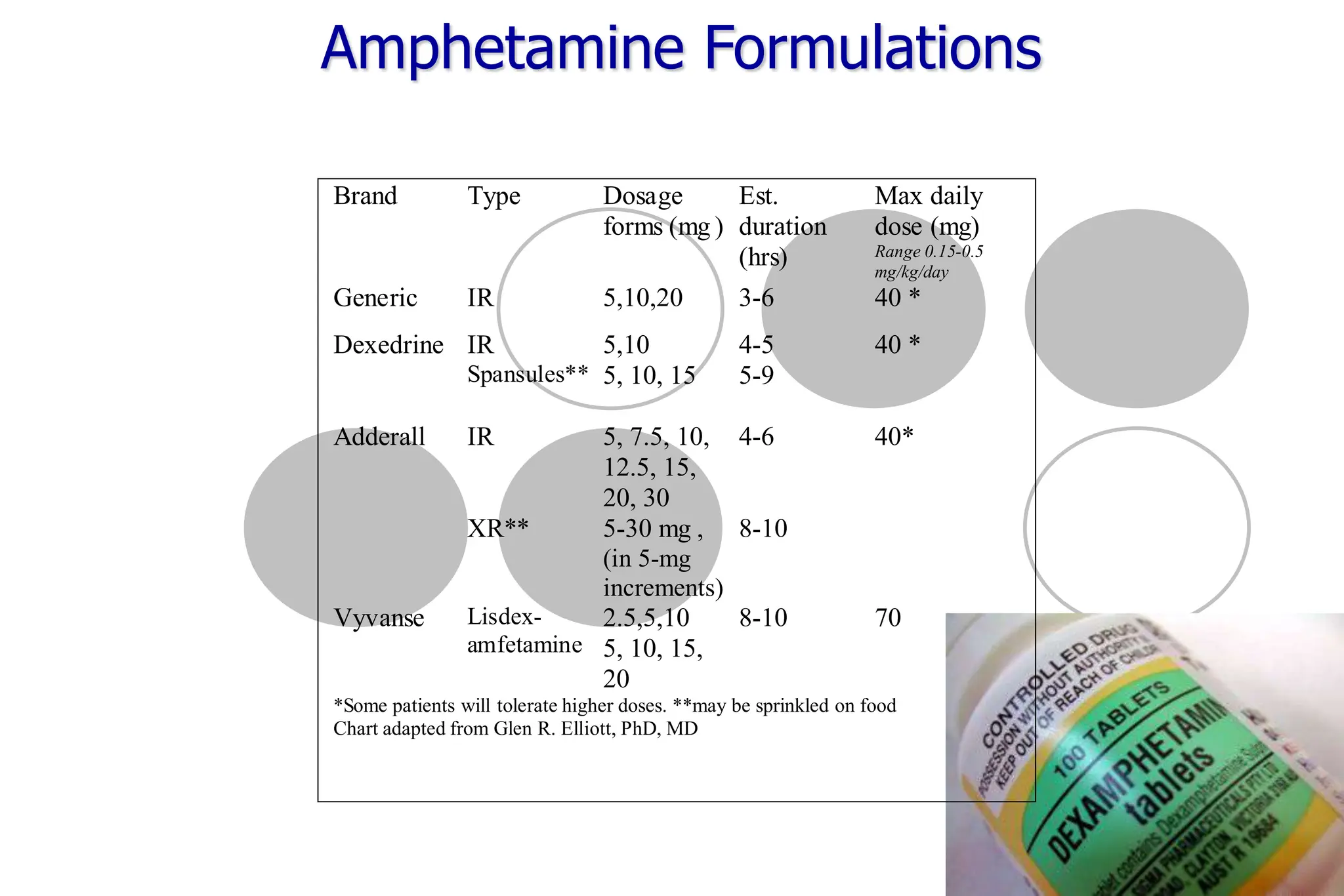
Methylphenidate Formulations
Brand Type Dosage
forms (mg )
Est.
duration
(hrs)
Max daily
dose [mg]
Range 0.3-
1.0mg/kg/day
Generic IR 5,10,20 2.5 - 4 [60]
Ritalin IR
SR
LA***
5,10,20
20
20
2.5 - 4
6 - ?
8-10
[60]
Methylin IR*
ER
5,10,20
5,10,20
2.5 - 4
6 -8
[60]
Focalin IR
XR***
2.5,5,10
5, 10, 15,
20
3-5
8-10
[20-30]
Metadate ER
CD***
10,20
20
6-8
8 -12
[60]
Concerta ER 18, 27,36,54 10 - 12 [72]
Daytrana patch 10, 15, 20, 3
0 9-12 [30]
[ ] Some patients may tolerate higher doses.
* Available in chewable tablets and liquid
*** May be sprinkled on food
Chart adapted from Glen R. Elliott, PhD, MD](https://image.slidesharecdn.com/adhdacrossthelifespan-240120164356-ed34cf68/75/ADHD-Across-the-Lifespan-ppt-39-2048.jpg)
















































![ADHD (best)]](https://cdn.slidesharecdn.com/ss_thumbnails/bykhaihojoshuagabriel1-1234763718979961-1-thumbnail.jpg?width=640&height=640&fit=bounds)