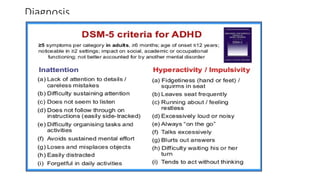
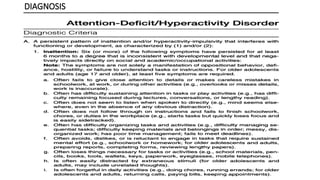
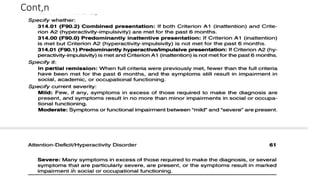
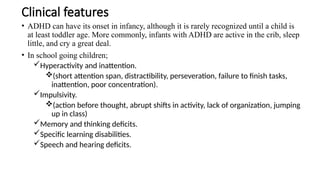
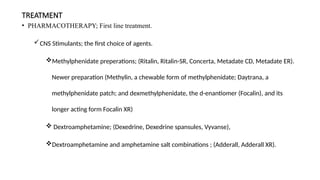
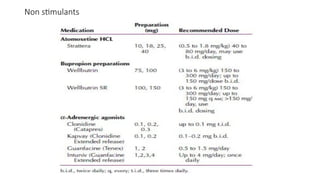
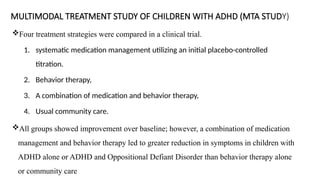
The document presents a comprehensive overview of Attention Deficit Hyperactivity Disorder (ADHD), detailing its definition, subtypes, epidemiology, etiology, diagnostic criteria, differential diagnoses, course and prognosis, and treatment options. ADHD is characterized by symptoms of inattention, hyperactivity, and impulsivity, impacting individuals' functioning across various life domains. The treatment involves pharmacotherapy and psychosocial interventions, with studies showing that combined approaches are the most effective.