Downloaded 804 times
![.
Extragenital:
. Endocrine: hypo or hyer thyroidism
. Haematological: Idiopathic thrombocytopenic
purpura, Von-Willebrand disease
. Chronic systemic disease: liver failure, renal failure,
hypertension with uterine artery atherosclerosis.
. Iatrogenic: Sex hormones, anticoagulants.
. Emotional: (change of country, climate & work;
stress; psychosomatic disorders)
. Obesity: [increased peripheral estrogen conversion]
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/aub-150708112051-lva1-app6892/85/Abnormal-uterine-bleeding-5-320.jpg)

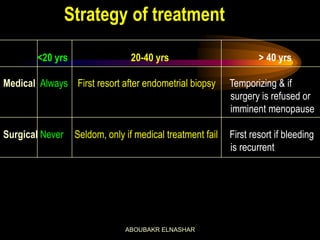




This document discusses abnormal uterine bleeding (AUB). It defines AUB and normal menstruation. It describes various clinical types of AUB and potential causes. Evaluation involves history, examination, and investigations. Treatment options include medical approaches like hormonal therapies and surgical procedures like endometrial ablation. Dysfunctional uterine bleeding is discussed in depth as the most common cause of AUB.























































































