Download to read offline


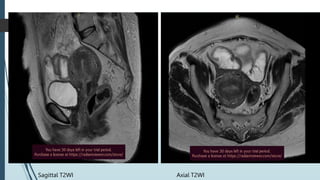
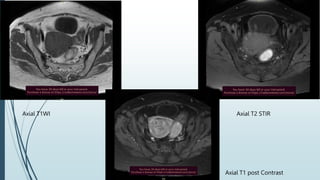
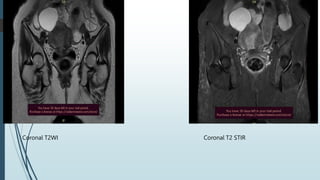
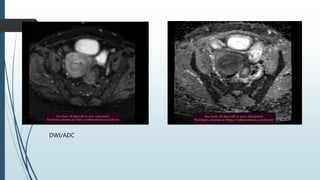


This MRI report describes findings for a 45-year-old woman with chronic pelvic pain. The MRI showed a bulky uterus with diffuse wall thickening up to 13 mm, consistent with adenomyosis. A well-defined cyst was also seen in the right adnexa. Adenomyosis is a common condition where endometrial tissue grows in the uterine wall and can cause symptoms like heavy periods. The MRI is helpful for diagnosing adenomyosis based on junctional zone thickening of 12 mm or more. In this case, the findings of diffuse uterine wall thickening and enhancement support a diagnosis of adenomyosis with an additional right adnexal cyst.































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)















