Downloaded 604 times








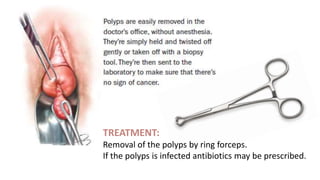


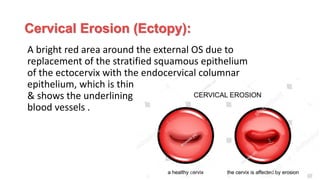



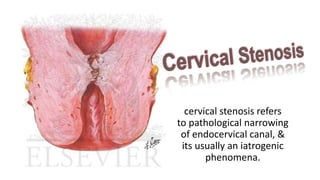
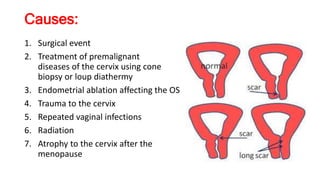













This document discusses several types of benign cervical lesions: - Cervical polyps are benign tumors arising from the endocervical epithelium that appear as smooth reddish protrusions. They are usually asymptomatic but can cause bleeding. Treatment involves removal by forceps. - Cervical ectropion (erosion) is the replacement of stratified squamous epithelium with columnar epithelium around the external cervical os. It has various causes and may cause discharge or bleeding. - Cervical stenosis is pathological narrowing of the endocervical canal, often due to prior surgical or medical treatments for premalignant cervical conditions. It can cause issues like hematometra or infertility. Treatment involves physically dil



































































