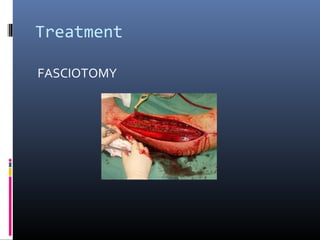
Compartment syndrome is a condition caused by increased pressure within a compartment of the body, limiting blood flow to tissues within that compartment. It has numerous potential etiologies including fractures, trauma, casts/dressings, and reperfusion injuries. The pathophysiology involves increased compartment pressure raising venous pressure and decreasing the arterial-venous gradient, causing ischemia of muscles and nerves. Diagnosis is based on history, clinical exam assessing the six Ps (pressure, pain, paresthesia, paralysis, pallor, pulselessness), compartment pressure measurements, and laboratory tests. Treatment involves lowering the affected limb, removing casts/dressings, and potentially performing an emergency fasciotomy to release pressure if clinical signs and pressures indicate ongoing ischemia



























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










