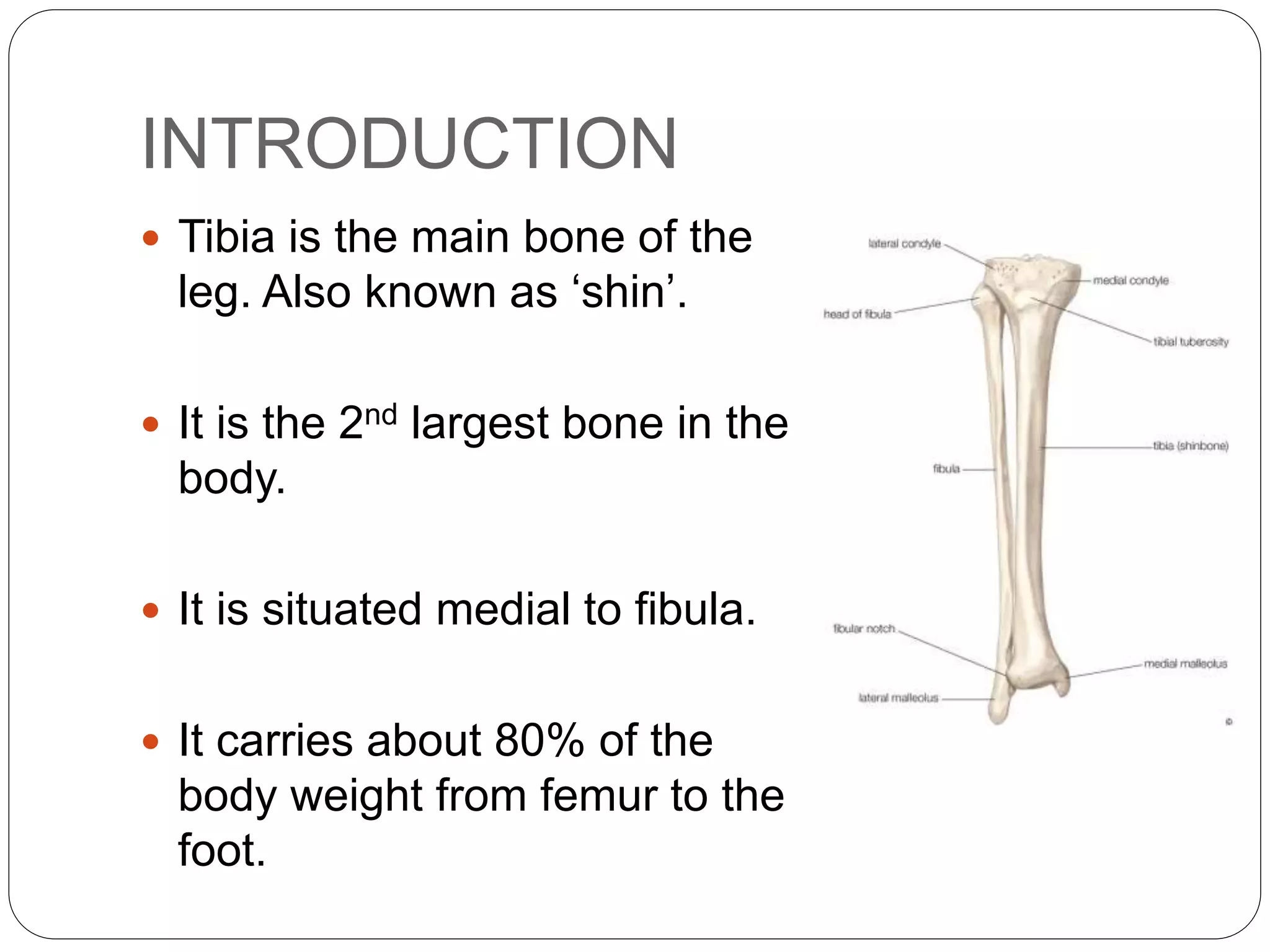
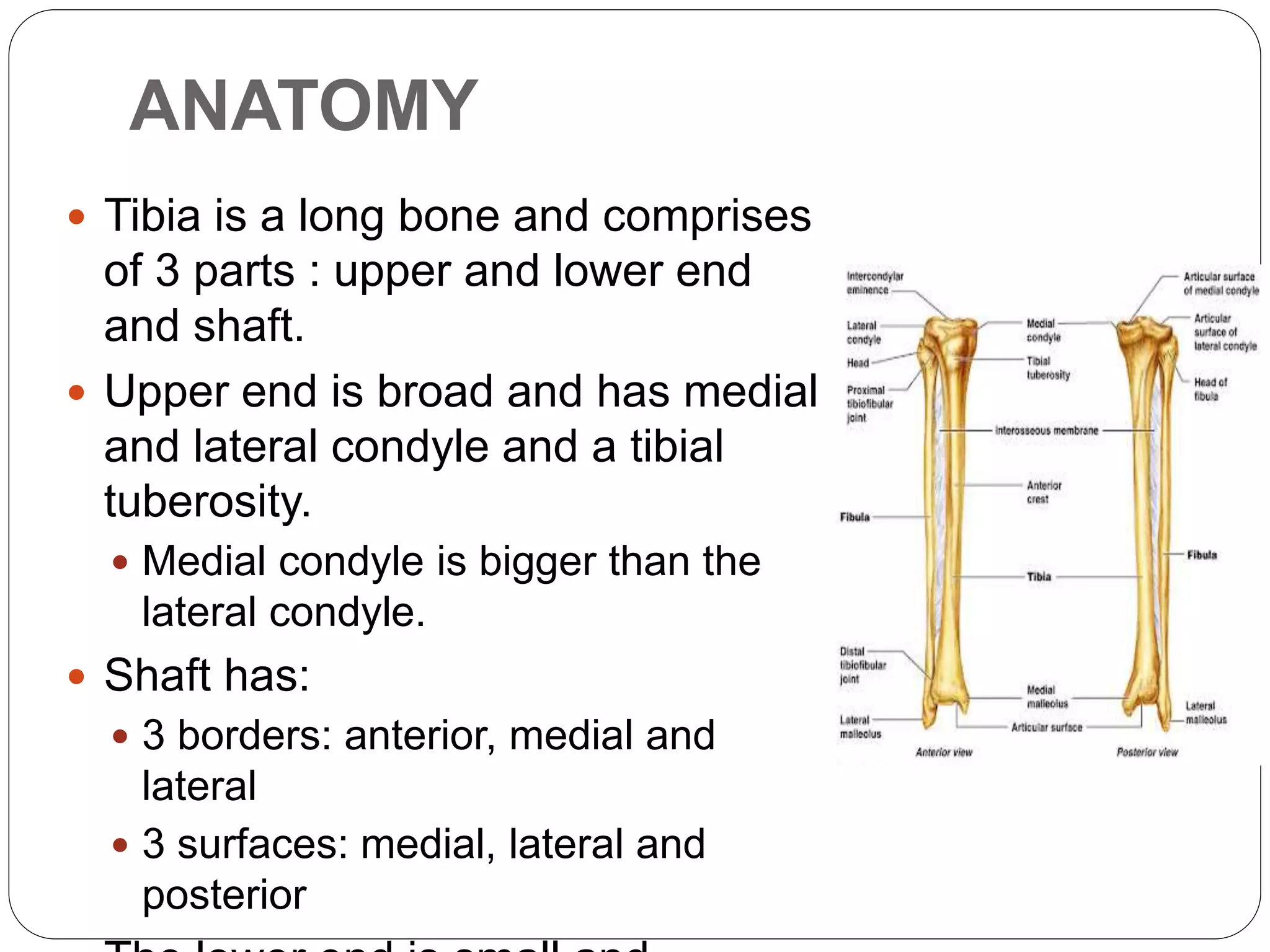
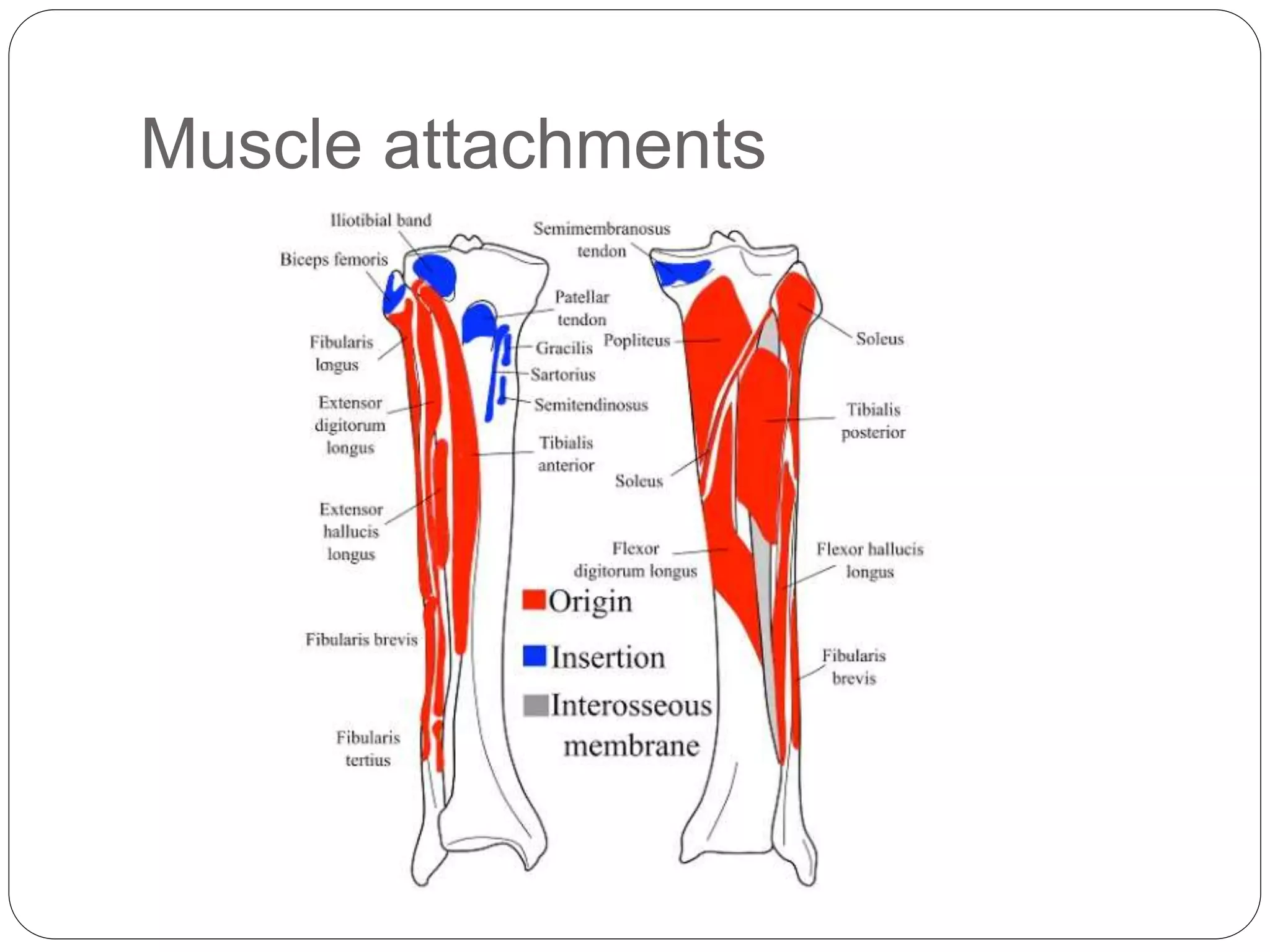
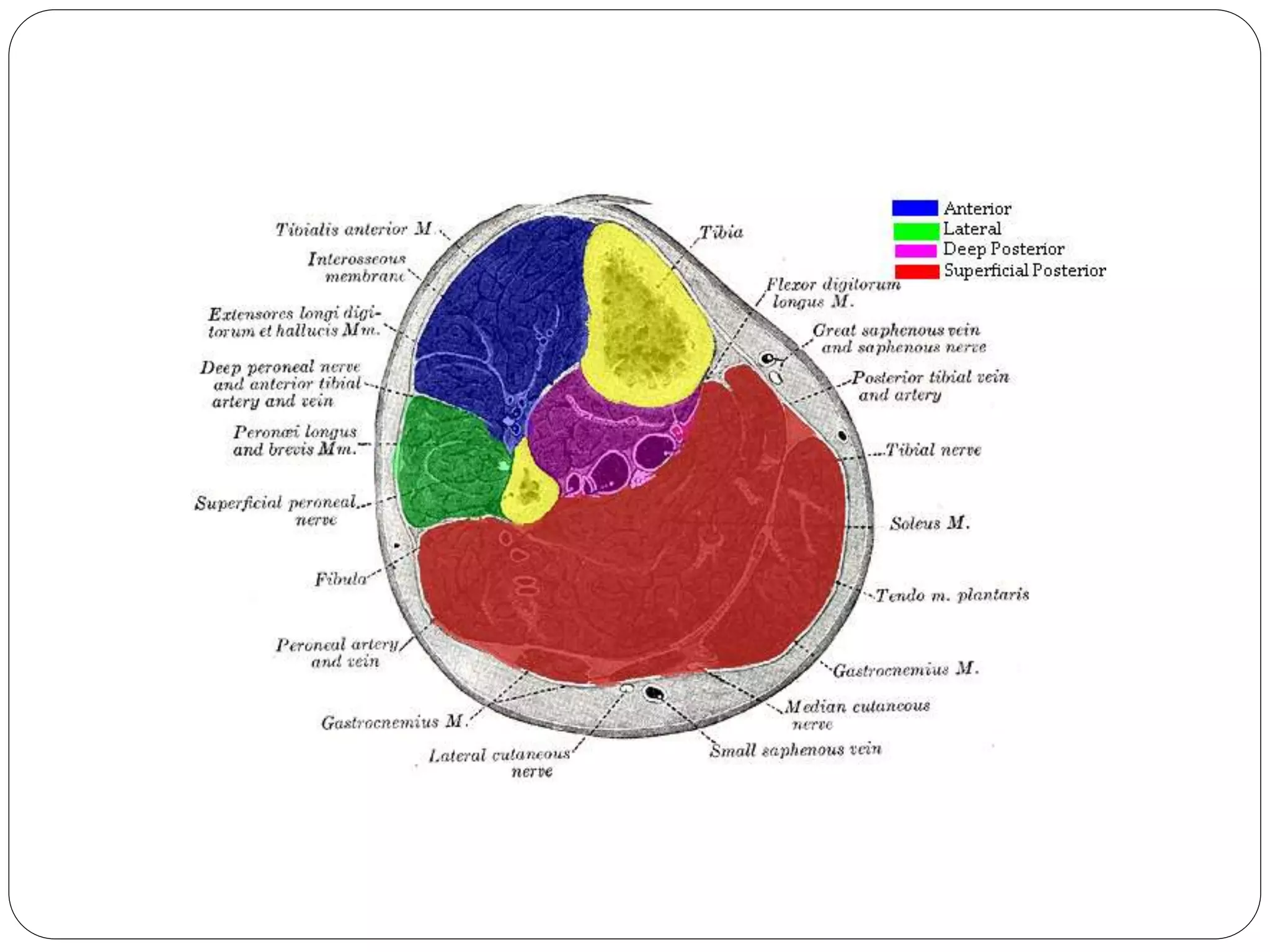
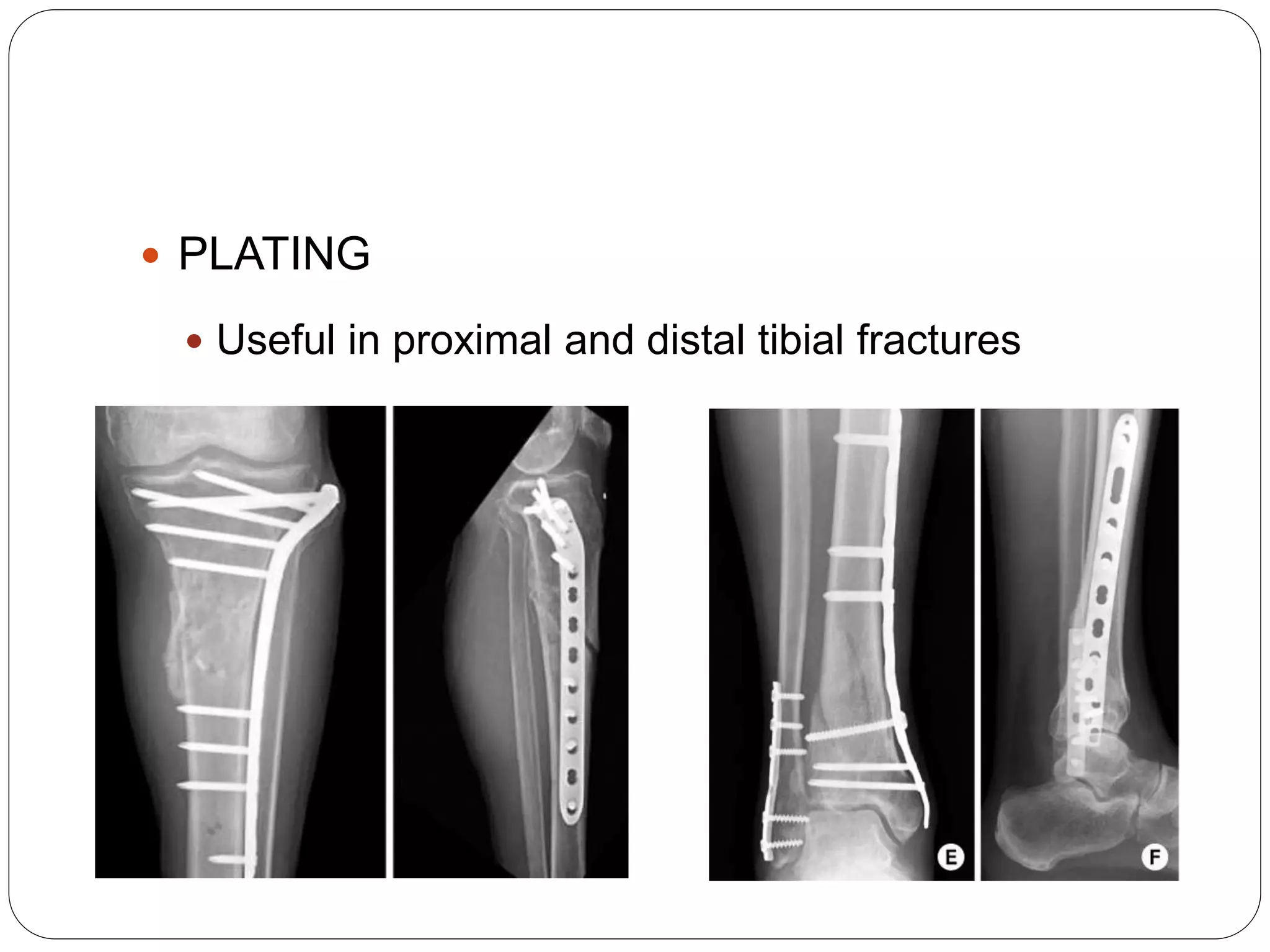
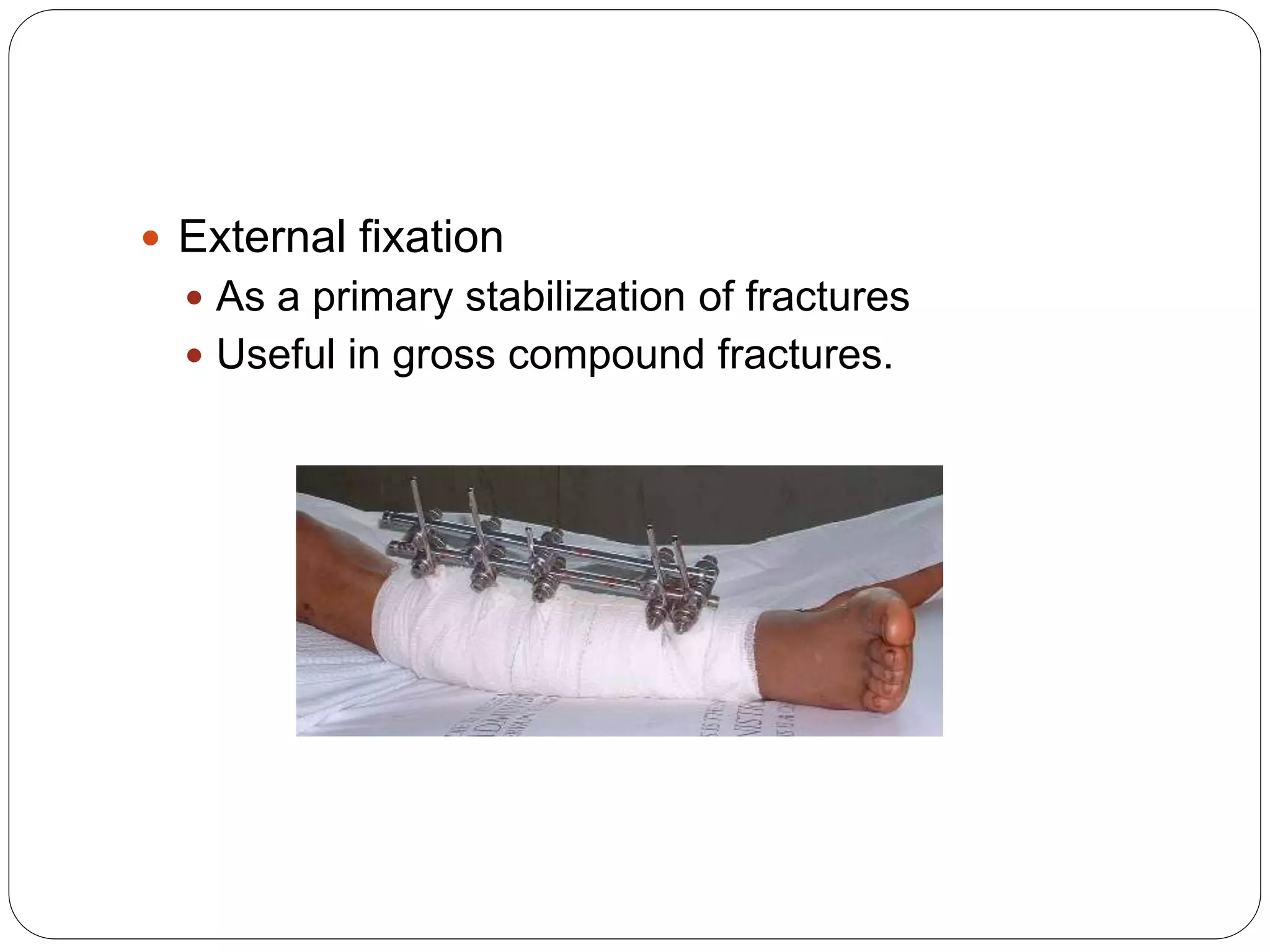
This document discusses fractures of the tibia shaft. It begins by providing an overview of tibia anatomy, noting that it is the second largest bone and carries 80% of body weight from the femur to the foot. It then describes the anatomy of the tibia in more detail. Mechanisms of tibia shaft fractures are discussed as well as common fracture patterns, clinical presentation, diagnostic imaging, and treatment approaches including non-operative and operative options like intramedullary nailing and plating. Compartment syndrome is also covered as a potential complication.