Downloaded 603 times
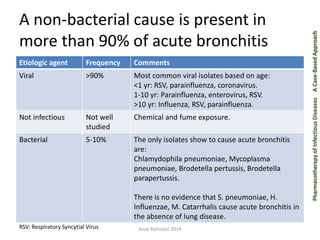
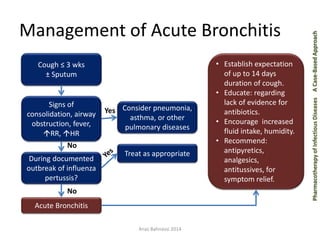
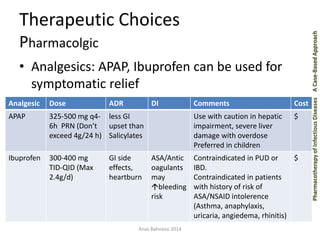
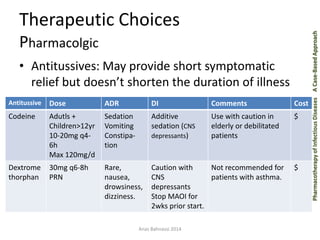
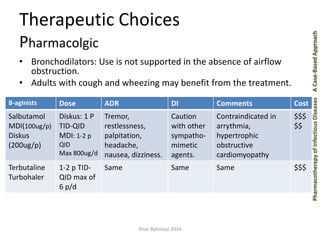


This document discusses the pharmacotherapy of acute bronchitis. It begins by defining acute bronchitis as a cough lasting less than 3 weeks, which is usually viral in origin. The goals of therapy are to rule out serious illness, minimize symptoms, and limit unnecessary antibiotic use. Treatment is primarily supportive and includes analgesics, antitussives, and bronchodilators only for those with wheezing. Antibiotics are not routinely recommended as they do not impact illness duration or severity. Education of patients about the typical self-limiting course of acute bronchitis is important.







































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















