Download as PDF, PPTX





















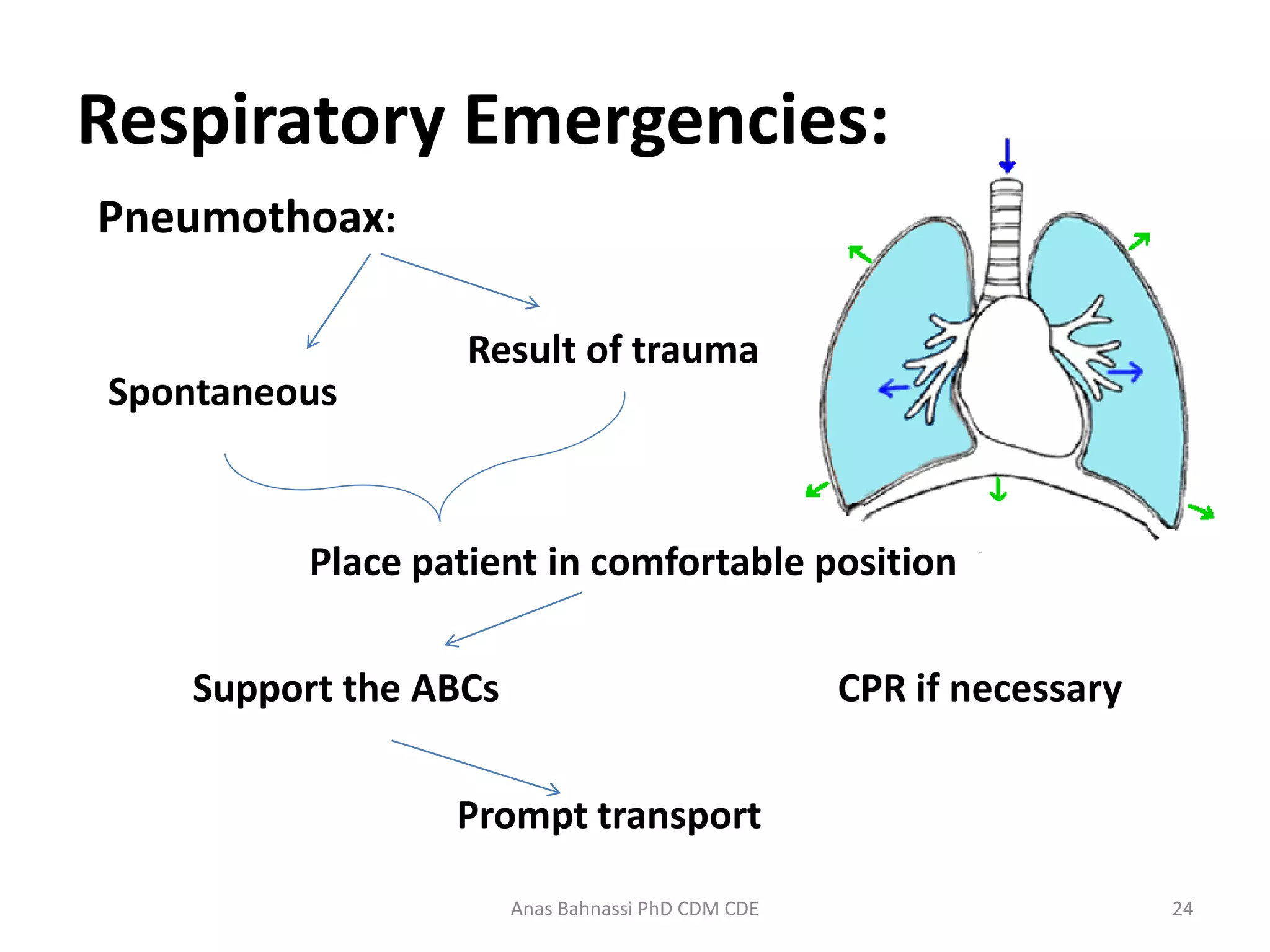


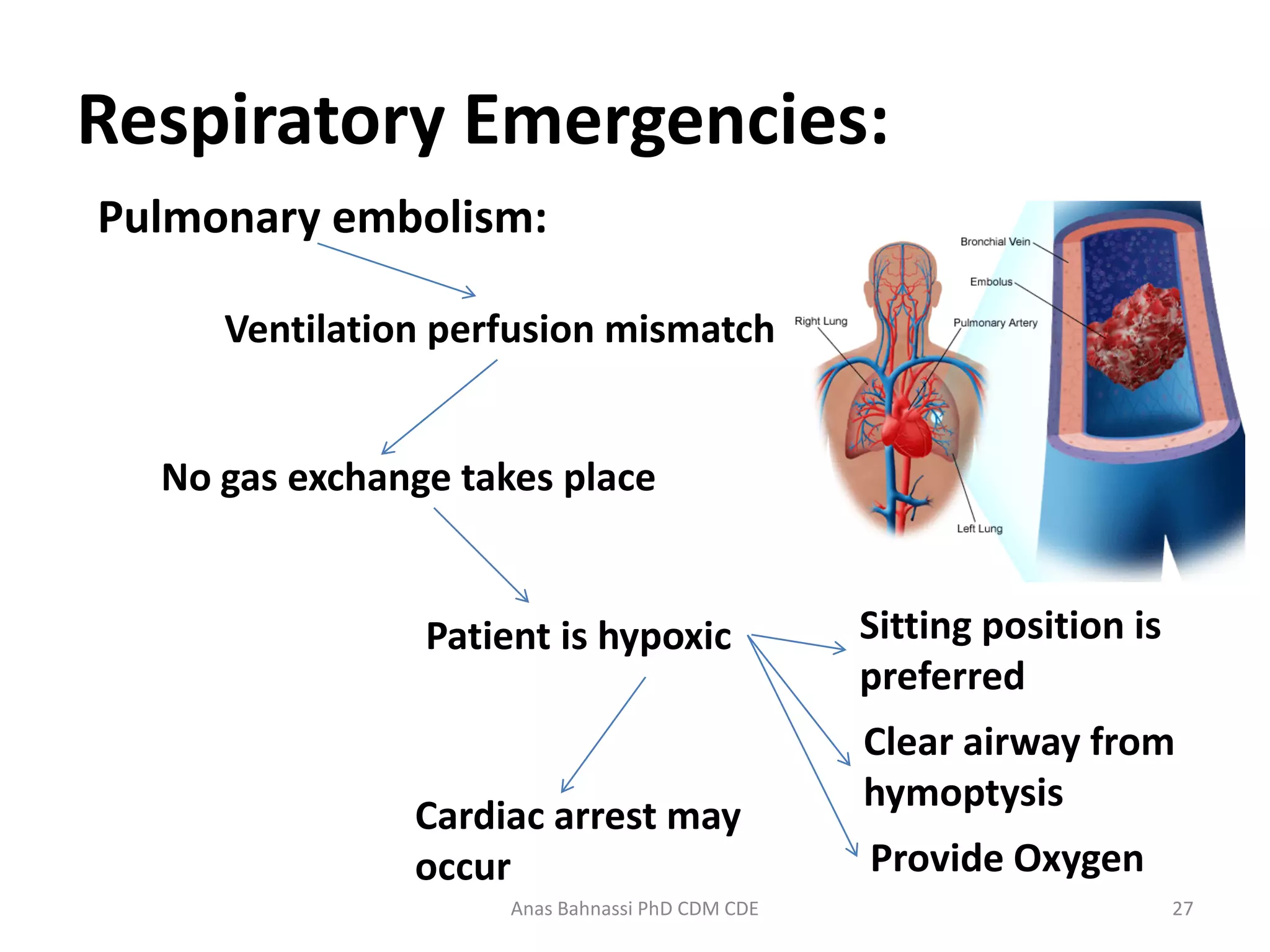



This document provides an overview of respiratory emergencies for emergency medical responders. It describes the anatomy and physiology of the respiratory system and signs of adequate versus inadequate breathing. It then details the primary, secondary, and reassessment phases for responding to a respiratory emergency including assessing the scene, airway, breathing, circulation, and vital signs. Specific conditions are covered such as upper airway infections, pulmonary edema, COPD, asthma, pneumothorax, pleural effusion, airway obstruction, pulmonary embolism, and hyperventilation. For each, the document outlines management steps like positioning, oxygen administration, ventilation support, and prompt transport.