Downloaded 26 times
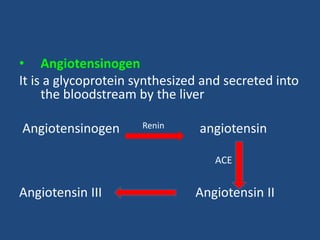
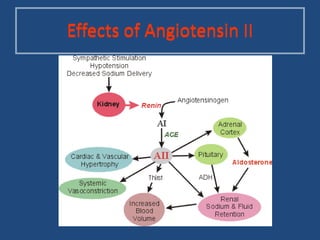
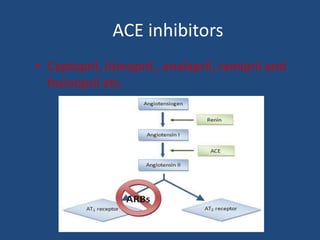



This document provides an overview of angiotensin-converting enzyme (ACE) inhibitors, including their indications, mechanisms of action, and evidence of effectiveness. ACE inhibitors are used to treat hypertension, congestive heart failure, myocardial infarction, diabetes, proteinuria, and other conditions. They work by inhibiting the conversion of angiotensin I to angiotensin II in the renin-angiotensin-aldosterone system. Clinical trials have shown that ACE inhibitors reduce blood pressure, prevent complications of heart failure and diabetes, and slow the progression of kidney disease. Common ACE inhibitors discussed include captopril, enalapril, lisinopril, and fosinopril.























































































