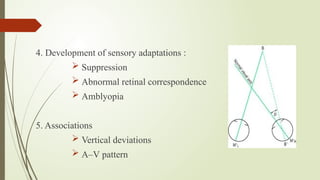
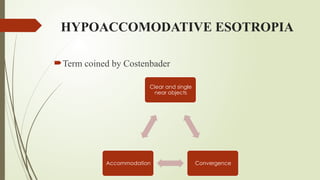
The document discusses accommodative esotropia, its classifications, prevalence, clinical features, and management strategies. It emphasizes the conditions under which esotropia occurs, its hereditary nature, and characteristics linked to refractive errors. Management options include optical corrections, amblyopia therapy, orthoptic exercises, and potential surgical intervention for associated deviations.






























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










