Downloaded 804 times






























The document provides an overview of psychological disorders including: - Historical models including the supernatural model which saw disorders as possession and the natural/medical model which saw them as diseases. - Modern models including psychoanalytic, biological, cognitive-behavioral, and diathesis-stress. - The DSM-IV-TR classification system and descriptions of mood disorders like depression and mania, anxiety disorders, psychosomatic disorders, dissociative disorders, sexual/gender disorders, and personality disorders. - Personality disorders are grouped into three clusters characterized by odd/eccentric, dramatic/erratic, and anxious/fearful behaviors respectively. Common disorders are described within each cluster.
Introduction to psychological disorders and defining abnormal vs normal behavior.
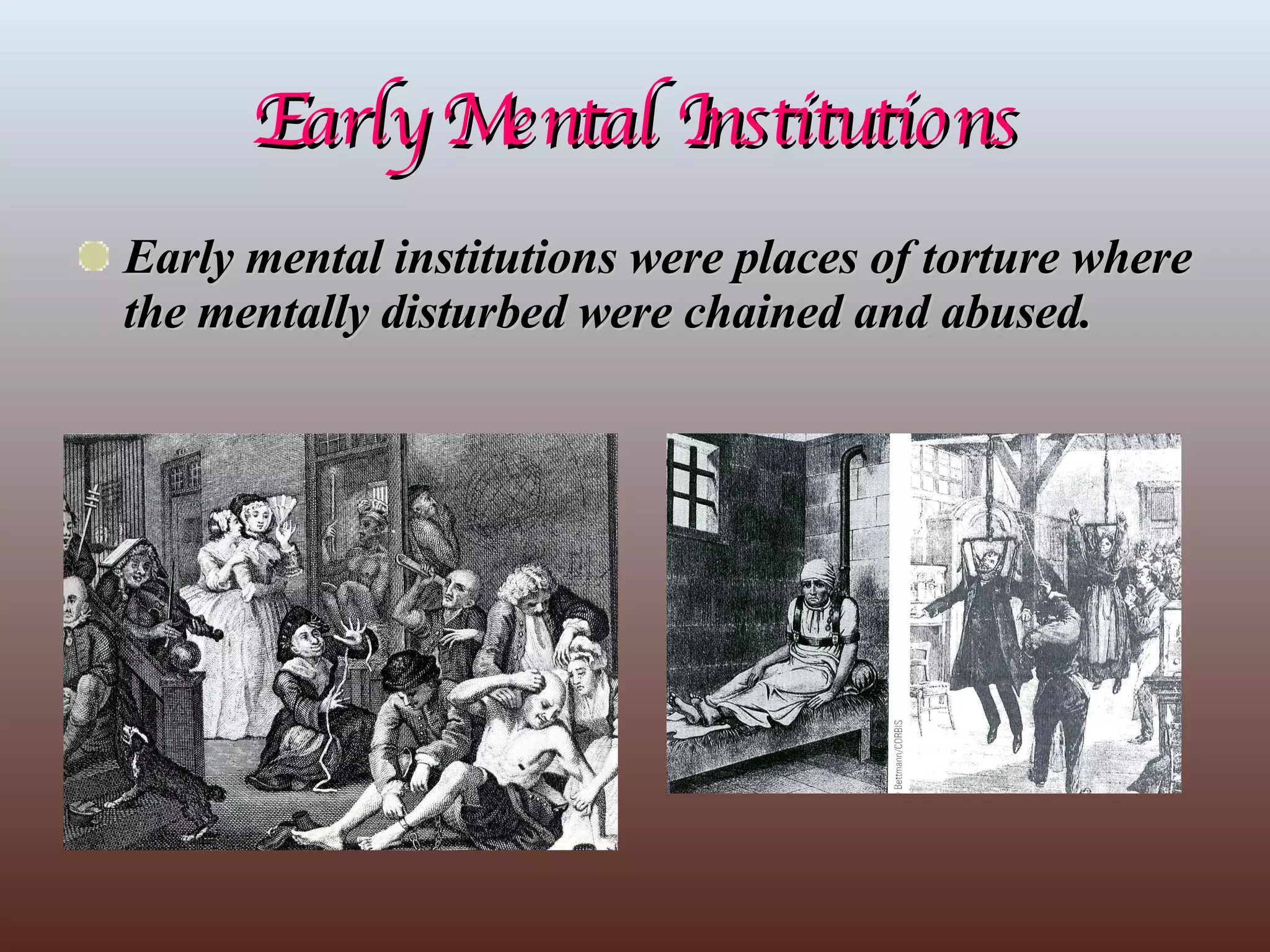
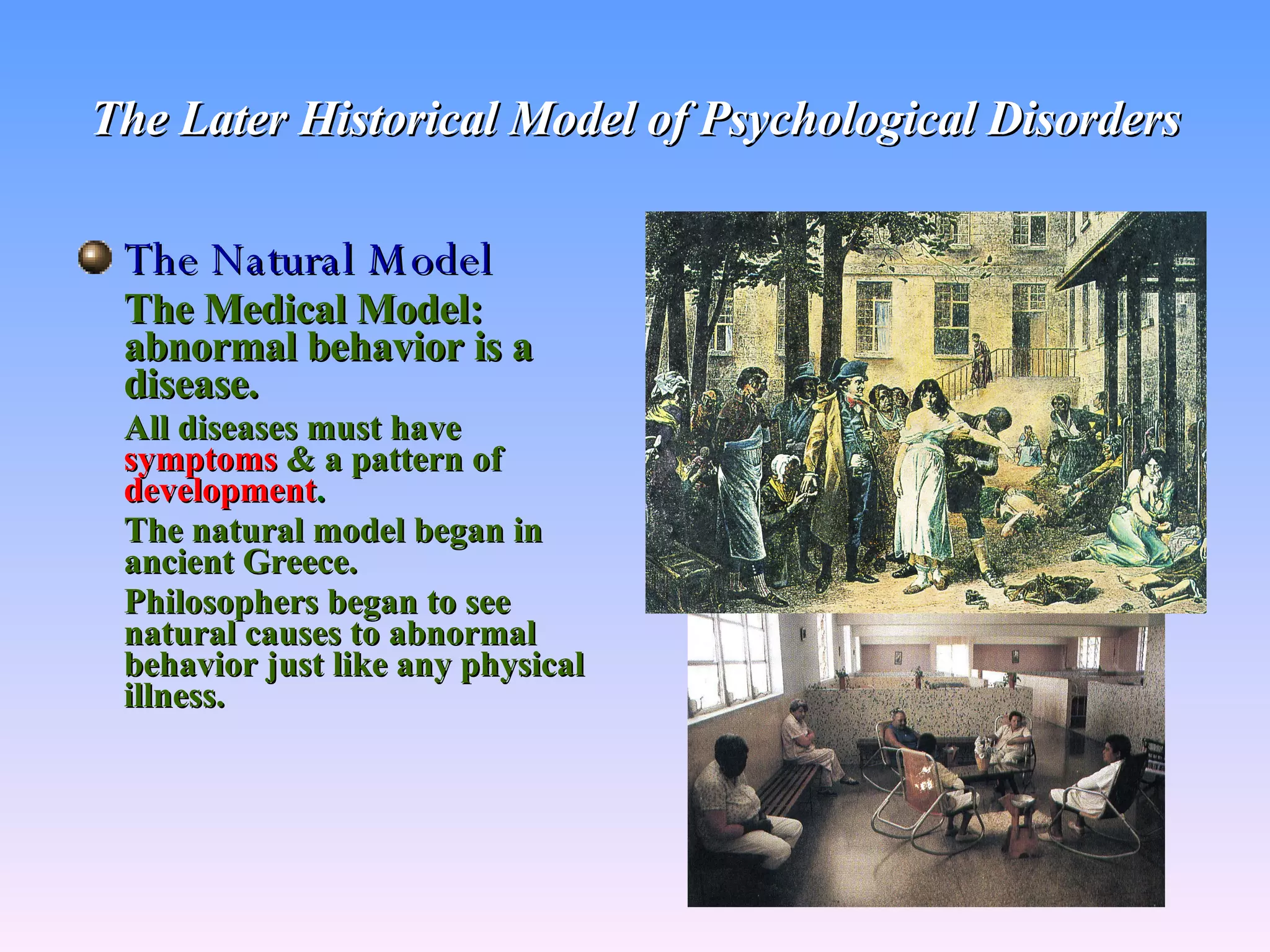
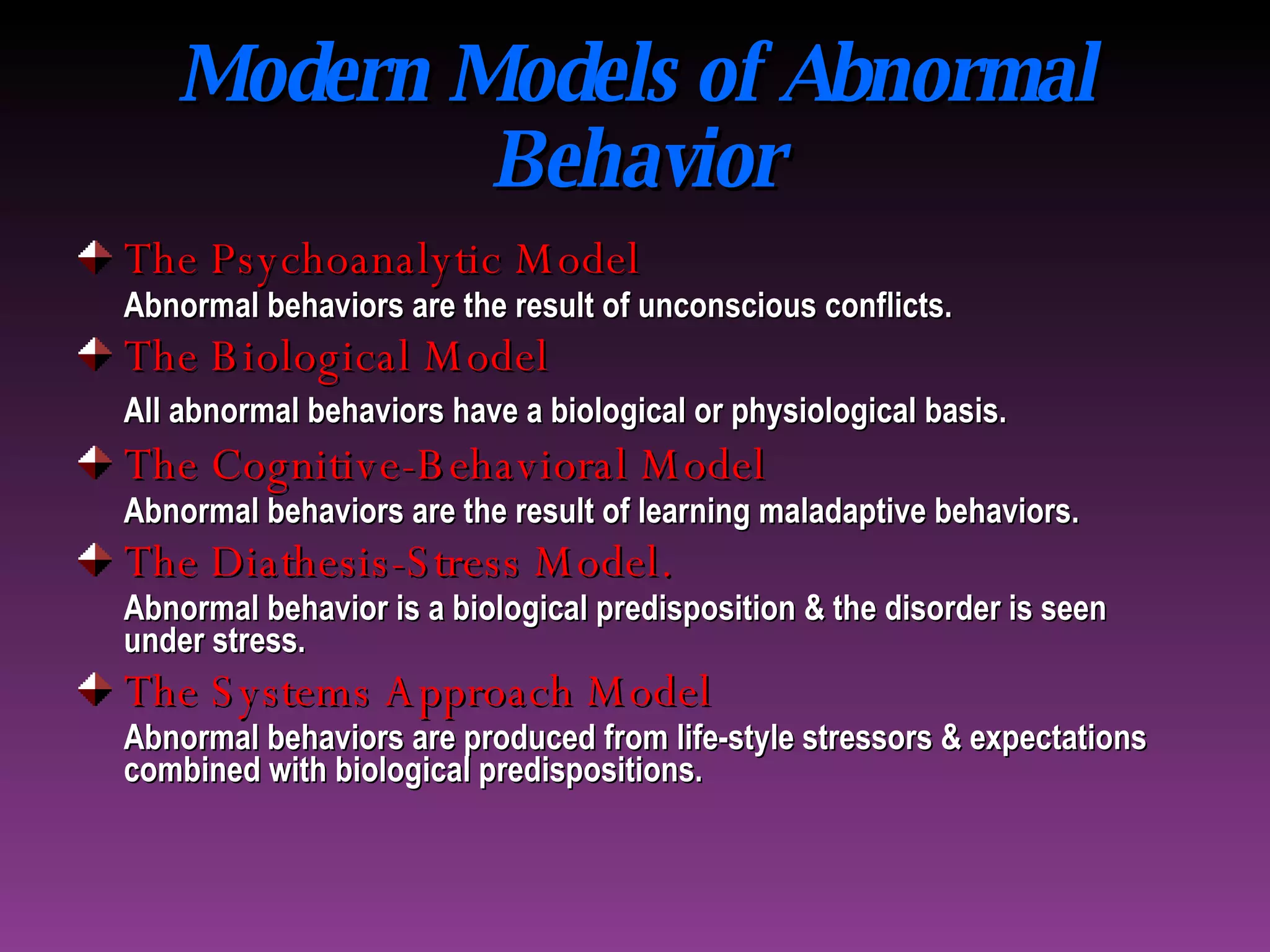
Overview of historical perceptions of psychological disorders, from supernatural to modern medical models.
Introduction to DSM-IV-TR and focusing on mood disorders, including definitions and types.
Insights into depression, its types, and causes; concerns around mania and its characteristics.
Description of anxiety disorders including definitions and types like GAD, OCD, and PTSD.
Insights into psychosomatic disorders, somatoform disorders, and dissociative disorders.
Overview of sexual dysfunctions and paraphilias including gender-identity disorders.
Description of various personality disorders grouped by characteristics and effects on behavior.
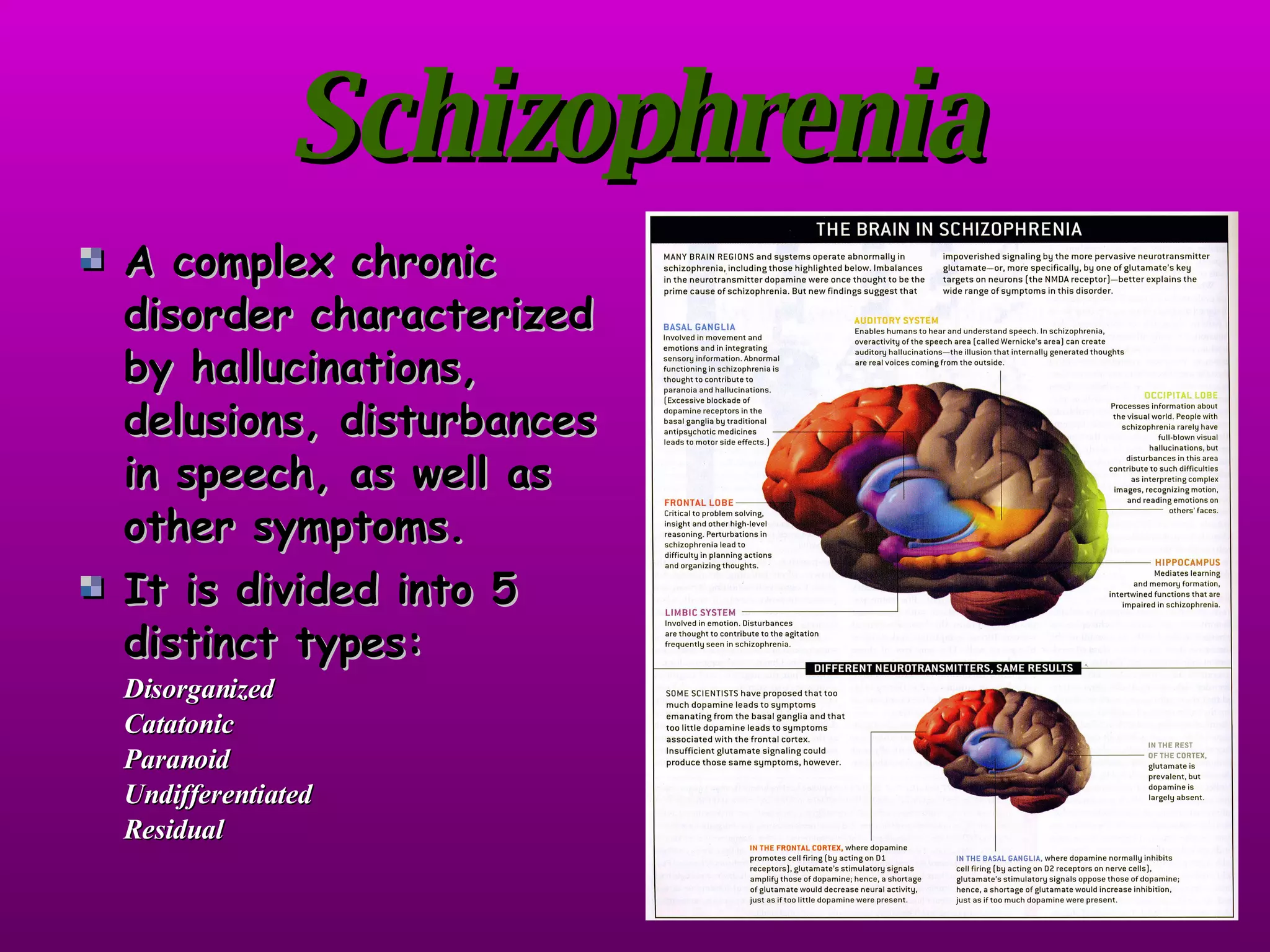
Insights into schizophrenia, its symptoms, types, and origins leading to understanding the disorder.
Discussion on age-related disorders such as Alzheimer's and Parkinson's and potential environmental causes.
Overview of childhood disorders like ADHD and autism, their characteristics, causes, and effects.