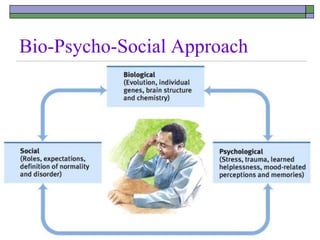
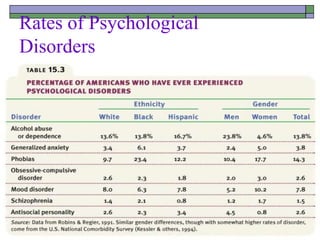
The document discusses psychological disorders, defining them as harmful dysfunctions that vary culturally and temporally, with diagnosis depending on symptom intensity and impact. It compares the medical model, which treats mental illnesses as diseases with physical causes, to the bio-psycho-social perspective, emphasizing a more holistic understanding of psychological disorders. Furthermore, it classifies types of psychological disorders such as anxiety, dissociative, personality, mood disorders, and schizophrenia while exploring their causes and characteristics.