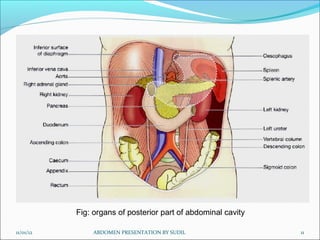
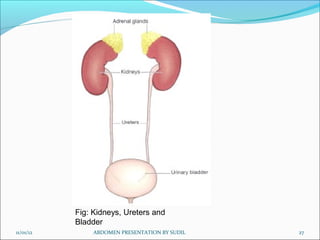
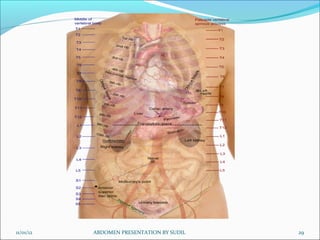
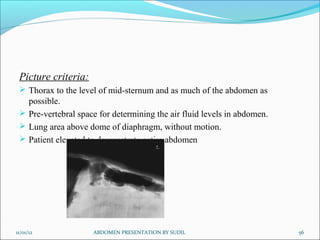
The document presents a detailed overview of the anatomy of the abdomen including its structure, divisions, contents, and relevant organs. It explains the abdominal wall, peritoneum, various organs such as the liver, pancreas, and kidneys, and the methods used for radiographic examination of the abdomen. Additionally, it covers the preparation and technique for abdominal radiography, including patient positioning and radiographic projections.












































































![5G Explained! A High Level Overview [Introduction]](https://cdn.slidesharecdn.com/ss_thumbnails/5gexplainedahighleveloverview-260119165306-cc137a3e-thumbnail.jpg?width=640&height=640&fit=bounds)














