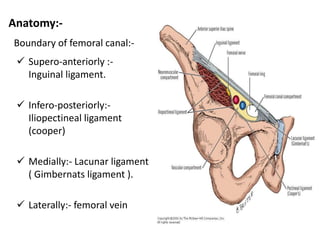
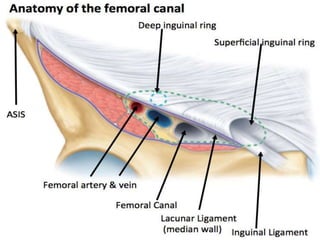
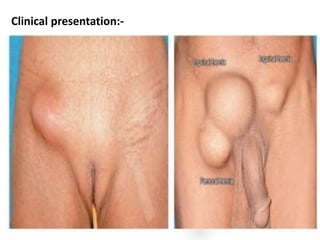
A 49-year-old female presented with a right inguinal swelling and pain for 15 days. On examination, a 2.5 x 2.5 cm globular swelling was found in the right femoral region that was firm, non-reducible, and dull on percussion. Ultrasound revealed a right femoral hernia. The patient underwent open surgery using the Lockwood approach under spinal anesthesia, which found a right femoral hernia containing 20 ml of peritoneal fluid. Femoral hernias occur when abdominal contents protrude through the femoral canal, presenting as a groin lump with exacerbated pain on bending or lifting. Diagnosis is made through history, exam, and ultrasound, with differential diagnoses including inguinal





























































![[MBBS/MS/DNB] Sample Long Case on Inguinal Hernia](https://cdn.slidesharecdn.com/ss_thumbnails/ccchernia-200501225130-thumbnail.jpg?width=640&height=640&fit=bounds)
















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


