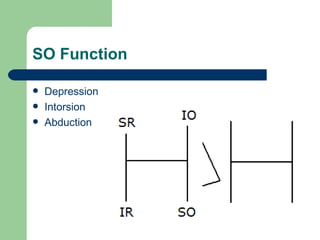
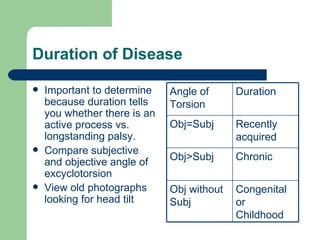
Superior oblique palsy is a weakness or paralysis of the superior oblique muscle, which functions to depress, intort, and abduct the eye. It causes double vision that is worse when looking in certain directions and may be accompanied by a compensatory head tilt. Diagnosis involves identifying which eye is higher in primary gaze, which eye shows worse deviation in right or left gaze, and which head tilt reduces the double vision. Causes can include trauma, congenital issues, ischemia, aneurysms, and tumors. Treatment may involve observation to see if it resolves on its own or use of prisms to reduce double vision.