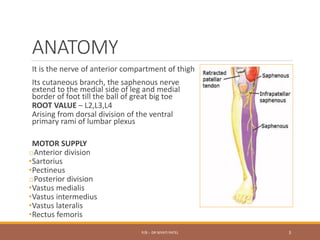
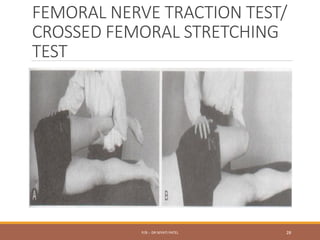
The femoral nerve originates from the lumbar plexus and innervates muscles in the anterior compartment of the thigh. Causes of femoral neuropathy include pelvic or femoral fractures, hip dislocations, spinal issues, and diabetes. Symptoms include sensory loss and weakness of the quadriceps and hip flexors. Special tests like the slump test and prone knee bending test isolate compression of the femoral nerve. Electromyography can help evaluate the severity and location of nerve damage. Treatment involves addressing the underlying cause, physical therapy, bracing, and surgery in severe cases.