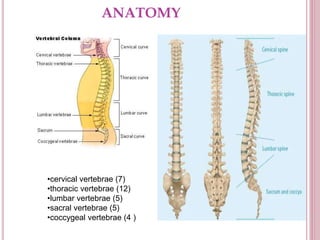
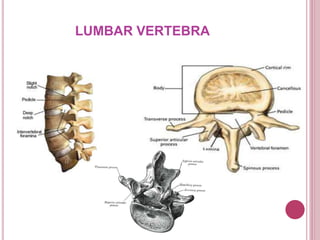
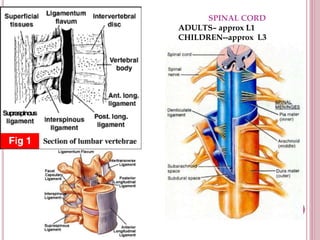
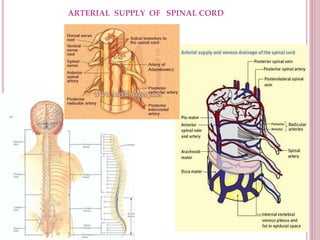
This document provides an overview of spinal and epidural anaesthesia. It discusses the anatomy of the spine and spinal cord, techniques for spinal and epidural anaesthesia including positioning and choice of local anaesthetics. It covers the physiological effects, common indications and contraindications. Potential complications are outlined along with their prevention and management. Overall, the document serves as a guide for the basic understanding and safe administration of spinal and epidural anaesthesia.
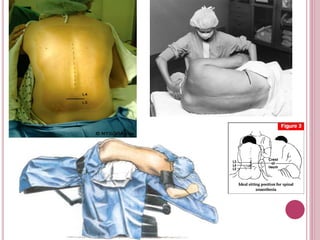
























































![Central neuraxial block in humans fcps[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/centralneuraxialblockfcps1-250708164057-daf1532a-thumbnail.jpg?width=640&height=640&fit=bounds)





































