


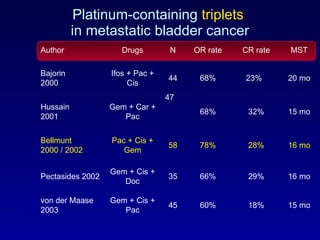
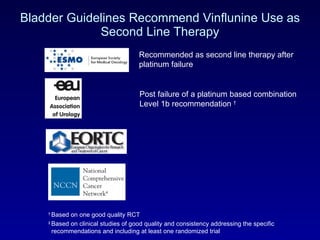
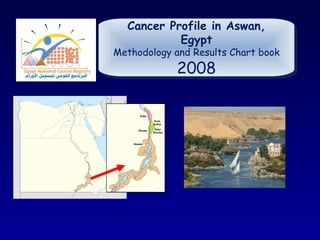
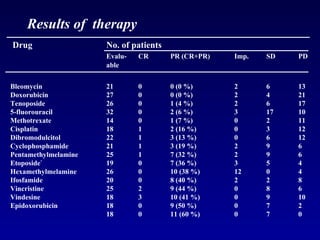
![Efficacy results * PS 0 = 320 mg/m²/q3w ** PS 0 with pelvic irradiation and PS 1 = 280 mg/m²/q3w Culine S et al. Br J Cancer. 2006 Vaughn DJ et al. Cancer. 2009 Culine et al. Vaughn et al. Number of treated patients n (%) 51 151 Initial dose (mg/m², q3w) 320 320*/280** Objective Response Rate n (%) 95% CI 9 (17.6) [8.4 - 30.9] 22 (14.6) [9.4 – 21.2] Disease control rate n (%) IRP 95% CI 34 (66.7) [52.1 - 79. 3 ] 86 (56.9) [48,7 - 65] Median Duration of response months IRP 95% CI 9.1 [4.2 - 15.0] 6.0 [5.4 – 9.5] Median PFS months 95% CI 3.0 [2.4-3.8] 2.8 [2.6 - 3.8] Median OS months 95% CI 6.6 [4.8 - 7.6] 8.2 [6.8 – 9.6]](https://image.slidesharecdn.com/4khaled-111130102001-phpapp01/85/H-Khaled-Bladder-cancer-State-of-the-art-56-320.jpg)

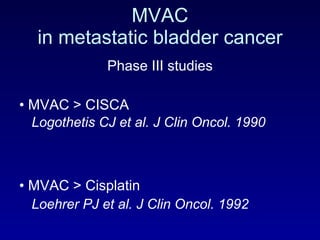
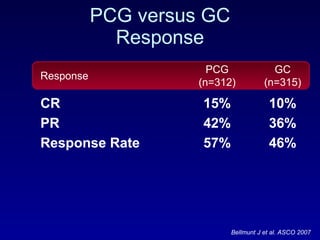
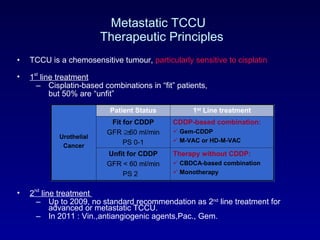
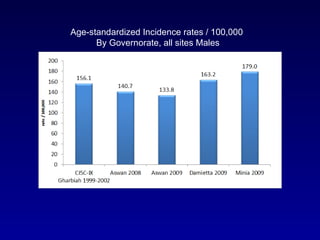
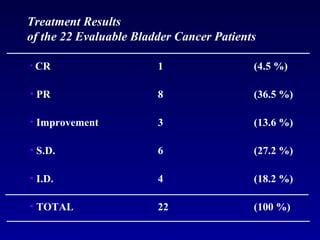
![> 3.5 -year follow-up Eur Urol Suppl. 2010;9(2):38 Updated survival analysis - ITT population VFL + BSC arm BSC arm 2.3 months Overall Survival [months]](https://image.slidesharecdn.com/4khaled-111130102001-phpapp01/85/H-Khaled-Bladder-cancer-State-of-the-art-58-320.jpg)



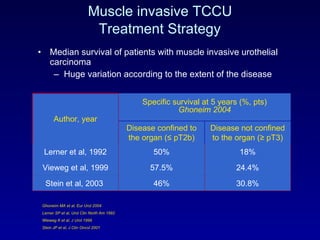
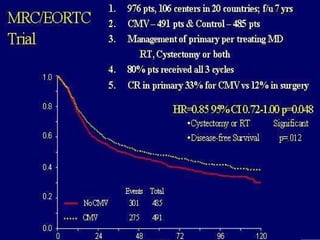









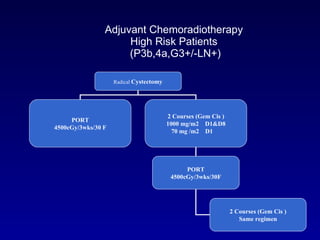



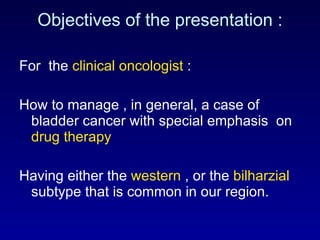
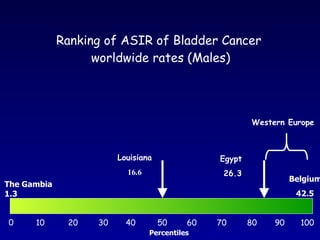
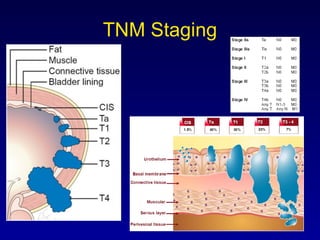
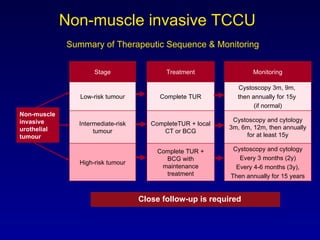
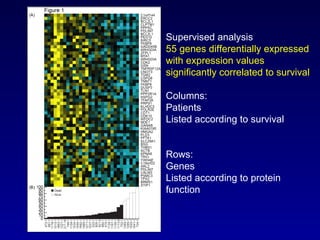
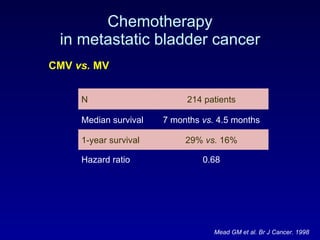
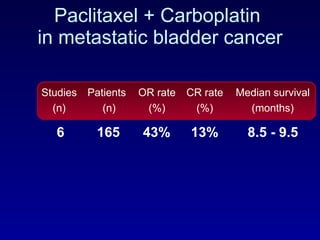
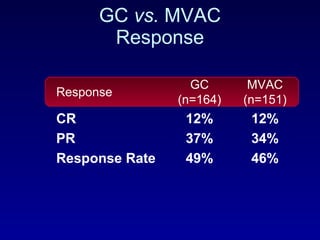
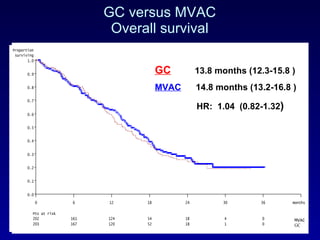
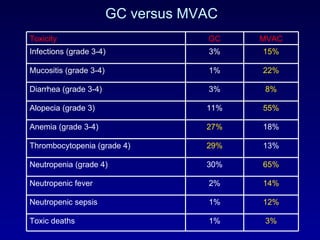
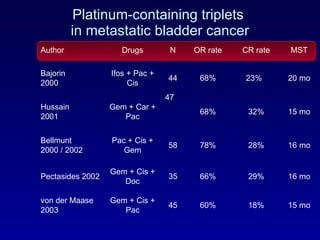
This document summarizes the management of urinary bladder cancer. It discusses staging, histopathologic types, and treatment options for non-muscle invasive and muscle invasive bladder cancer as well as metastatic disease. Standard first-line chemotherapy for metastatic bladder cancer includes gemcitabine and cisplatin or MVAC. Newer chemotherapy regimens and agents are also discussed.





































![Bladder Cancer NMIBC [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/non-muscleinvasivebladdertumoredmond-140716212950-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

![Muscle invasive bladder Cancer [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/muscleinvasivebladdertumoredmond-140716213247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



































































