Bladder Cancer Guidelines
ABrief Review
Waleed A. Hassen M.D.
Chairman of Urology
Tawam Hospital
Assistant Professor
Johns Hopkins Medical Institutions
Understanding Pathology
WHO/ISUP 1998 Consensus WHO 2004
• Papilloma
• Papillary urothelial neoplasm of low
malignant potential (PUNLMP)
• Urothelial Carcinoma low-grade
• Urothelial Carcinoma high grade *
– Previously classified grade 2 now high grade
4.
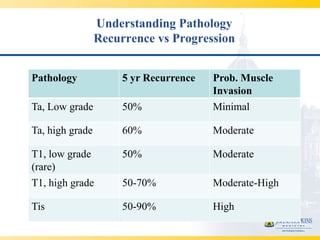
Understanding Pathology
Recurrence vs Progression
Pathology 5 yr Recurrence Prob. Muscle
Invasion
Ta, Low grade 50% Minimal
Ta, high grade 60% Moderate
T1, low grade 50% Moderate
(rare)
T1, high grade 50-70% Moderate-High
Tis 50-90% High
5.
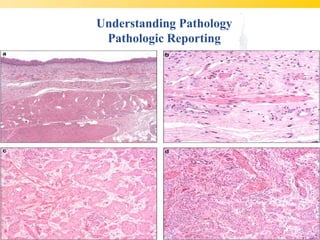
Understanding Pathology
Pathologic Reporting
• Pathology report must comment:
– Histologic grade
– The presence of muscularispropria, and degree
of involvement
– Presence or absence of LVI
– Presence or absence of CIS
Staging
• Suspect MuscleInvasive Disease
– CBC, Chemistry including AlkPhos
– CXR or CT Chest
– Upper tract imaging
– CT or MRI
– Bone Scan if Alk. Phos elevated or symptoms
10.
Transurethral Resection
• Goalsof TUR:
– Complete resection of all visible tumor when
possible
– Adequate mapping of bladder if needed
– Adequate staging by ensuring presence of
muscle
11.
Management
• cTa (lowgrade)
– Complete resection
– Observation vs single dose intravesical
chemotherapy*
12.
Management
• cTa (highgrade)
– Complete resection
– Re-resection if no muscle in specimen*
– Induction Immunotherapy
– Chemotherapy only if unable to tolerate BCG
13.
Management
• cT1 (highgrade)
– Complete resection
– Strongly advise re-resection
– Consider early cystectomy especially if re-
resection shows higher stage or volume disease
– Induction BCG otherwise
– Chemotherapy only if unable to tolerate BCG
14.
Restaging TURBT
• 150cases who underwent re-staging
TURBT
• Residual disease found in 76% Patients
• Upstaging to muscle invasive disease in 30% of
patients who initially had superficial disease
• Results are similar when same surgeon
performs resection
15.
Management
• cTis
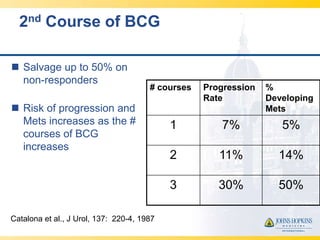
– Induction Immunotherapy
– If response consider maintenance BCG
• (x 3 years)
– Recurrent or persistent CIS, consider
cystectomy after no more then 2 courses of
BCG
Management
– cT2
• Radiation concomitant with chemo therapy
– No hydronephrosis
– Repeat TUR and boost to 65Gy if negative
– Simulate/treat patient with empty bladder
– High recurrence rate
• Radiation alone in patients with extensive co-
morbidities
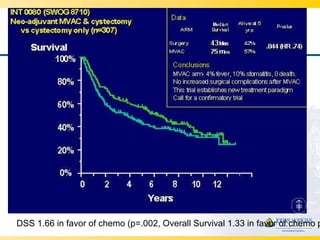
DSS 1.66 infavor of chemo (p=.002, Overall Survival 1.33 in favor of chemo p
28.
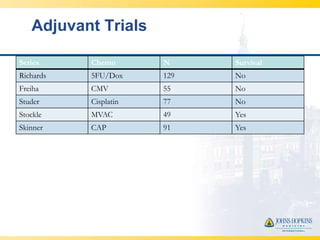
Adjuvant Trials
Series Chemo N Survival
Richards 5FU/Dox 129 No
Freiha CMV 55 No
Studer Cisplatin 77 No
Stockle MVAC 49 Yes
Skinner CAP 91 Yes
29.
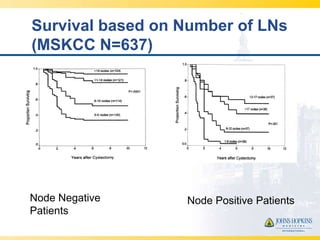
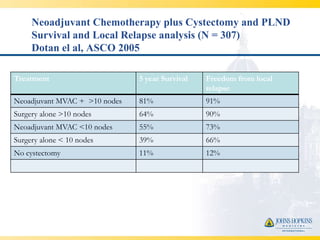
Neoadjuvant Chemotherapy plusCystectomy and PLND
Survival and Local Relapse analysis (N = 307)
Dotan el al, ASCO 2005
Treatment 5 year Survival Freedom from local
relapse
Neoadjuvant MVAC + >10 nodes 81% 91%
Surgery alone >10 nodes 64% 90%
Neoadjuvant MVAC <10 nodes 55% 73%
Surgery alone < 10 nodes 39% 66%
No cystectomy 11% 12%
30.
Management
– Metastatic Disease
• Gemcitabine/Cisplatin preferred
– Equivalent efficacy to MVAC
• 3 drug regimens have not been shown to be more
efficacious
• Carboplatin is NOT a substitute for Cisplatin
– Consider split dose cisplatin for borderline renal function
• Consider Carboplatin or Taxane-based regimens for
patients not candidates for Cisplatin
31.
Management
– Bladder canceris a lifelong disease
– Attention to published surveillance protocols
– Attempt multi-disciplinary care whenever
possible
– Do not forget about upper tracts