Downloaded 75 times
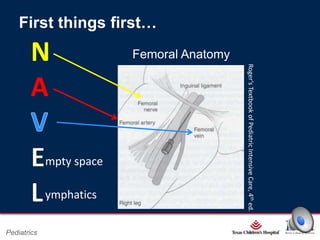
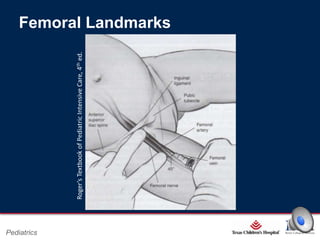
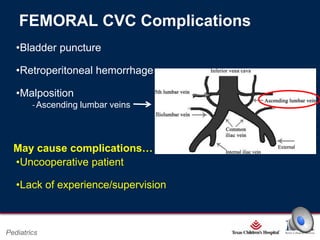
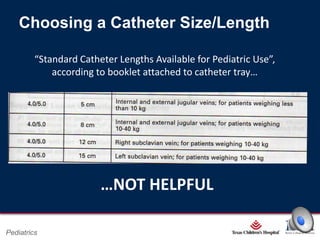
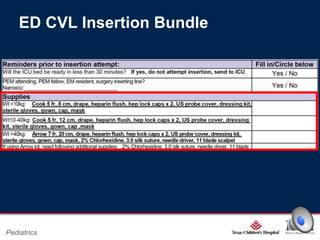


This document provides an overview and refresher on central venous catheterization procedures for pediatric patients. It outlines the objectives of learning how to combine ultrasound guidance with landmark techniques for femoral catheter placement. It reviews femoral anatomy, indications and contraindications for catheterization, potential complications, and how to select an appropriately sized catheter. The document emphasizes following a checklist and bundle for sterile technique when performing ultrasound-guided femoral central line insertions in pediatric patients.
































































































