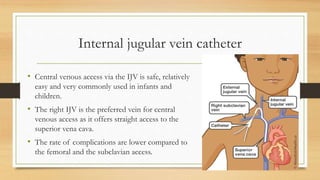
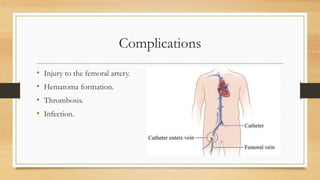
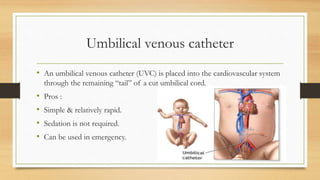
This document discusses vascular access considerations for neonates and pediatric patients requiring dialysis. It notes that peritoneal dialysis is generally preferred for these populations. The ideal vascular access provides adequate flow, long lifespan, and low complication rates, with arteriovenous fistulas best meeting this definition but not always feasible for small children. It then reviews various central vascular access options like catheters placed in the internal jugular, subclavian, and femoral veins. It provides guidance on catheter sizes, insertion techniques, potential difficulties, and complications for each approach. Peripherally inserted central catheters and umbilical venous catheters are also summarized.

























![Crrt indications and modalities [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/crrtindicationsandmodalitiesautosaved-181208052139-thumbnail.jpg?width=640&height=640&fit=bounds)






























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









