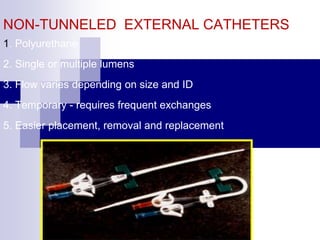
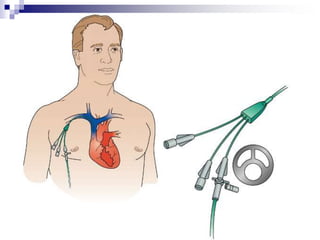
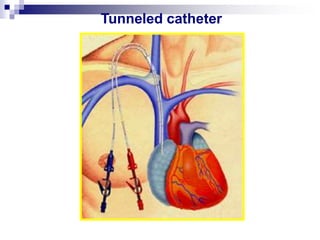
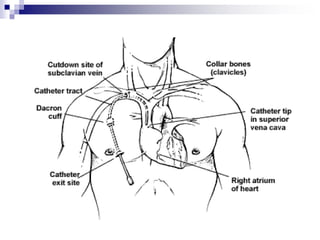
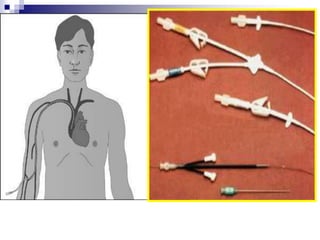
The document provides information on inserting and caring for peripheral IV lines and central venous catheters. It discusses choosing appropriate equipment, insertion sites, known complications, and general nursing care to minimize risks. Peripheral IVs are used for short-term therapy while central lines can be non-tunneled, tunneled, PICCs, or ports, depending on the anticipated length of treatment and patient's condition. Ongoing care includes dressing changes, flushing lines, and monitoring for complications like infection, phlebitis, occlusion or extravasation.