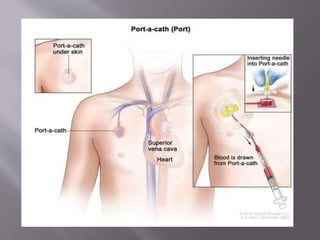
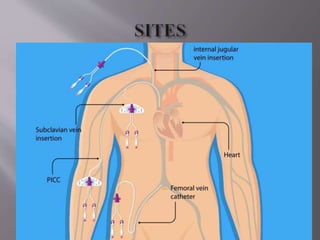
This document discusses central venous catheters. It describes central lines as flexible tubes inserted into large veins near the heart to deliver fluids, medications, blood products, and monitor central venous pressure. It outlines different types of central lines including non-tunneled, tunneled, and implanted ports. The document discusses indications, contraindications, complications, and proper insertion and maintenance techniques to prevent infections like chlorhexidine skin antisepsis and dressing changes. The goal is to promote infection prevention best practices for central lines.