
Download to read offline
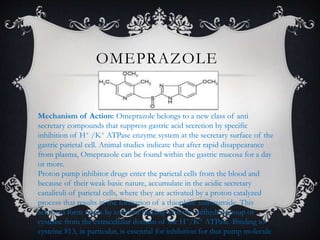

1) Proton pump inhibitors like omeprazole, lansoprazole, pantoprazole, rabeprazole, and esomeprazole are widely used to treat gastric acid-related disorders by inhibiting the H+/K+ ATPase pump in parietal cells. 2) They work by accumulating in the acidic canaliculi of parietal cells where they are activated and bind covalently to cysteine residues on the pump, irreversibly inhibiting it. 3) Common side effects include headache, diarrhea, abdominal pain, and nausea. They generally have few drug interactions but some are metabolized by CYP450 enzymes and may






















































































