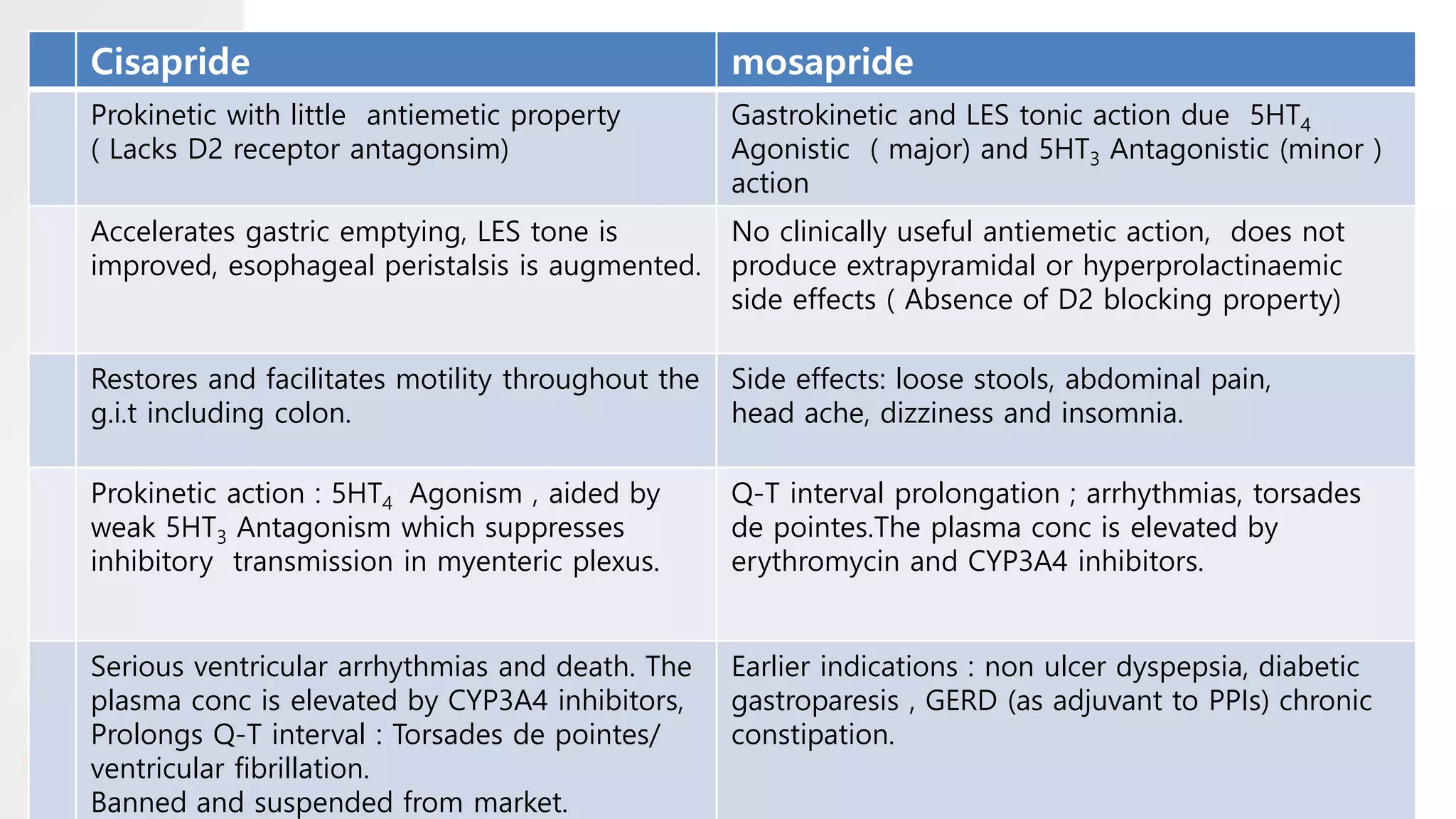
Prokinetic drugs enhance gastrointestinal motility by increasing the frequency and strength of contractions, aiming to alleviate symptoms such as abdominal discomfort and nausea. Key prokinetics include metoclopramide, domperidone, and cisapride, each with varying mechanisms and side effects. While they are valuable in treating conditions like gastroesophageal reflux disease and gastroparesis, some, like cisapride, have been banned due to severe side effects.











































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)








