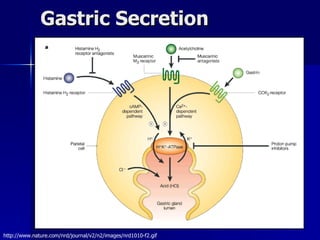
1) The document discusses medications used to treat gastrointestinal disorders by suppressing acid secretion or affecting gastrointestinal motility. It covers proton pump inhibitors, H2 receptor antagonists, antacids, and other drugs used for conditions like GERD, ulcers, constipation, and diarrhea.
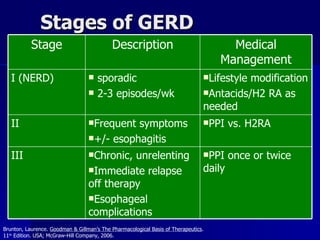
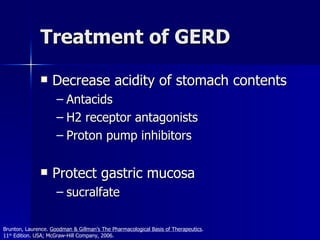
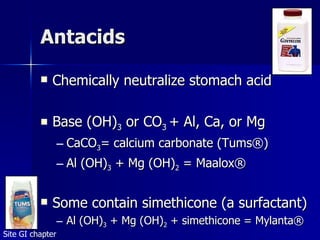
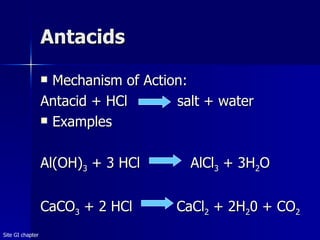
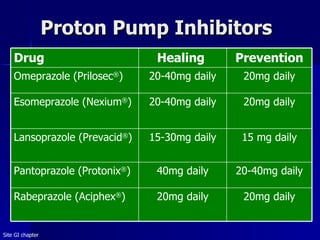
2) Specific drugs are highlighted for treating acid reflux including PPIs like omeprazole, H2 blockers like ranitidine, and antacids. Treatment for H. pylori infection and complications of long-term acid suppression are also reviewed.
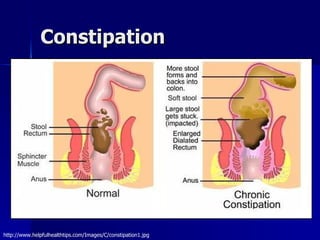
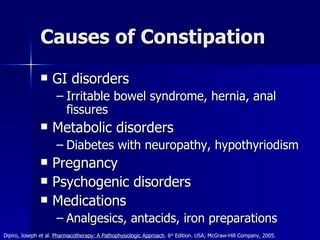
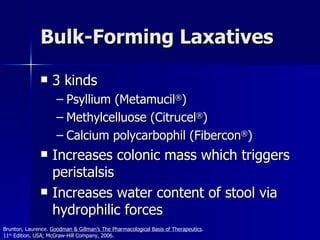
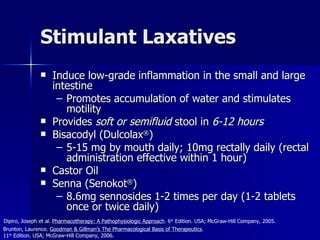
3) Laxatives for constipation are categorized and specific examples given for each type. Opioid derivatives and adsorbents are outlined