Downloaded 22 times

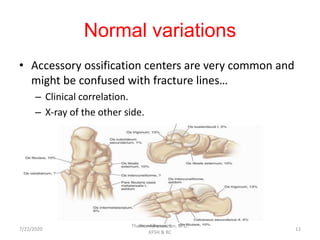
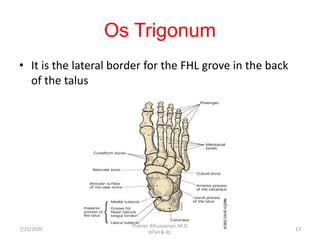

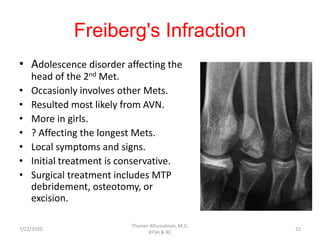
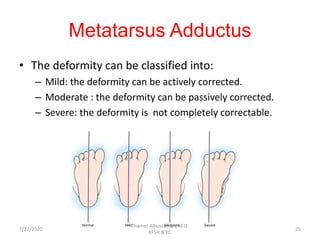
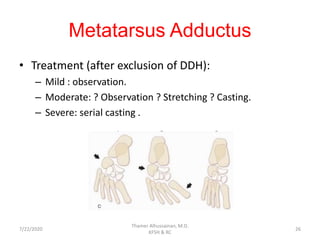
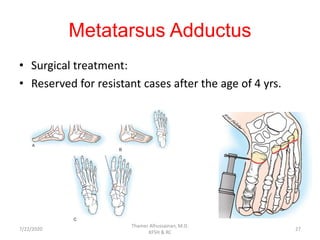
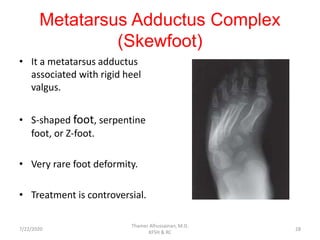
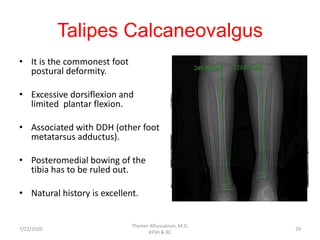


The document provides an introduction to pediatric foot conditions. It discusses the anatomy and development of the pediatric foot. It then covers normal variations that can occur, including accessory ossification centers. Two common osteochondroses - Köhler's disease and Freiberg's infraction - are described. Several congenital and developmental foot deformities are outlined, including metatarsus adductus, talipes calcaneovalgus, flexible flatfoot, and tarsal coalition. Treatment approaches for many of these conditions are mentioned, with an emphasis on conservative care.